While bacteria cause immunologic glomerular injury and glomerulonephritis, this topic is not discussed here (see Chapter 10).
TABLE 24.1 Clinical syndromes of acute pyelonephritis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
situation. There is an increased prevalence of asymptomatic bacteriuria in older patients; in men, it is commonly caused by prostatic enlargement and loss of bactericidal activity of prostatic secretions (17). Poor bladder emptying due to uterine prolapse is considered important in women (18,19). Neuromuscular disease, increased instrumentation, and catheter use contribute in both sexes. Asymptomatic bacteriuria, or asymptomatic UTI, is defined by the U.S. Preventive Services Task Force as isolation of a specified quantitative count of bacteria in an appropriately collected urine specimen obtained from a person without symptoms or signs referable to urinary infection (20). Asymptomatic bacteriuria is due to bacteria that lack virulence factors (discussed under pathogenesis).
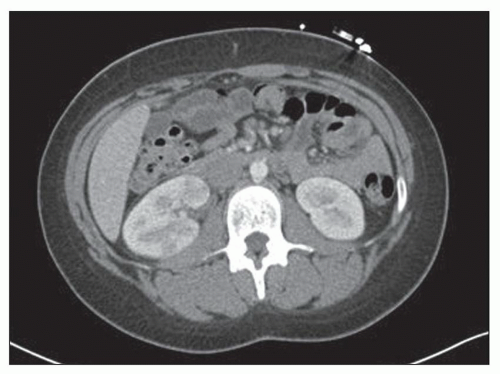 FIGURE 24.1 Contrast-enhanced transverse CT shows multiple wedge-shaped areas of lower attenuation with effacement of the corticomedullary junction in the right kidney. These findings are highly suggestive of pyelonephritis. (Courtesy of Cary Siegel, Mallinckrodt Institute of Radiology, St. Louis, Missouri.) |
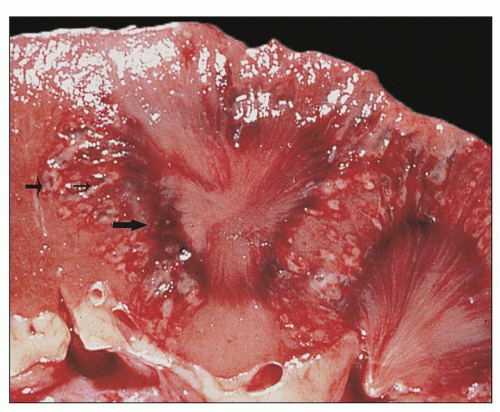 FIGURE 24.2 Acute pyelonephritis. Cortical abscesses are apparent and straight yellow streaks (thin arrows) and hyperemia in the medulla (thick arrow). |
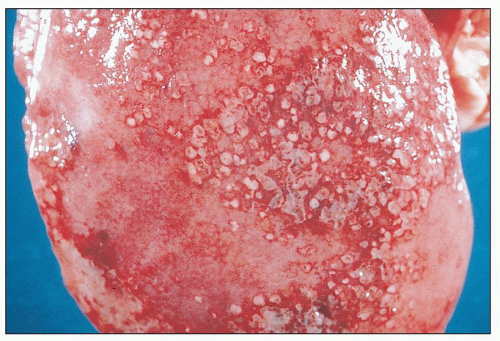 FIGURE 24.3 Acute pyelonephritis. Cortical abscesses produce discrete or confluent, raised, yellowish-white, rounded nodules with surrounding hyperemia on the subcapsular surface. |
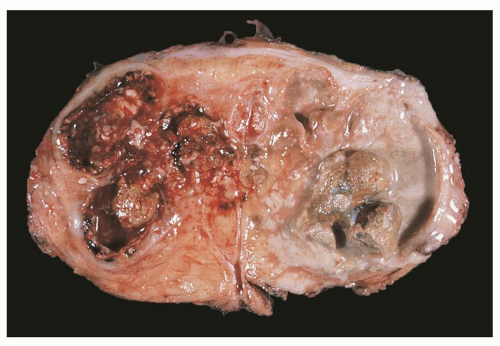 FIGURE 24.4 Pyonephrosis. The kidney is converted into a pus-filled sac, with little identifiable parenchyma. The mucosa of the collecting system is focally hemorrhagic and covered by creamy exudate; it contains several calculi. |
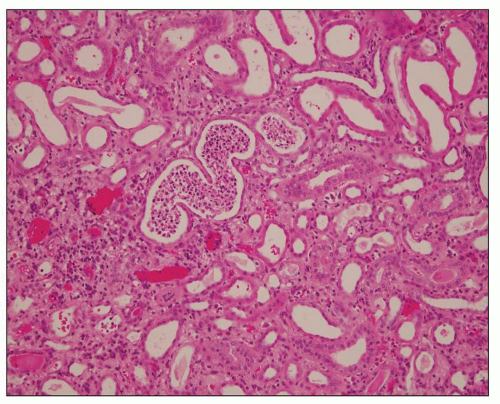 FIGURE 24.5 White cell casts in acute pyelonephritis. (H&E; ×400.) |
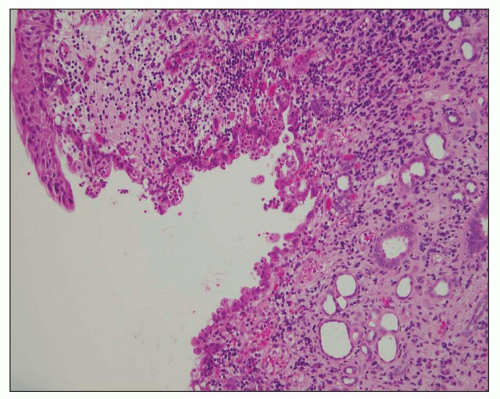 FIGURE 24.6 Acute pyelitis; neutrophils erode the lining epithelium forming microabscesses. (H&E; ×200.) |
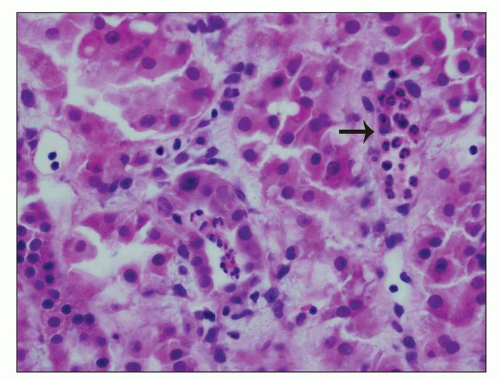 FIGURE 24.7 In acute pyelonephritis, neutrophils appear first in peritubular capillaries (arrow). (H&E; ×400.) |
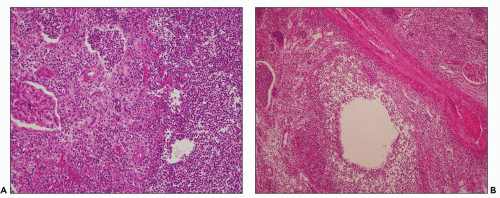 FIGURE 24.8 Acute pyelonephritis. A: Pools of neutrophils destroy tubules; glomeruli are remarkably unaffected. B: Abscess formation. (H&E; ×200.) |
and neutrophil recruitment to the kidney, which may worsen renal injury, but there is considerable controversy on the pathology of ATN in humans compared to animal models (38). Recent studies suggest that interstitial injury activates innate immunity and the inflammasome, a new concept to explain inflammatory responses in kidney disease in various conditions including ATN and obstruction (39,40). Innate immune response in the context of kidney infection is discussed further under pathogenesis of pyelonephritis.
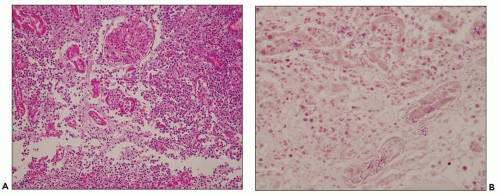 FIGURE 24.10 Suppurative pyelonephritis from a 68-year-old man with diabetic end-stage kidney disease. A: Massive neutrophil influx obscures and destroys proximal tubules. (H&E; ×200.) B: Gram-negative bacteria admixed with neutrophils in tubules and the interstitium. (Gram stain × 400.) |
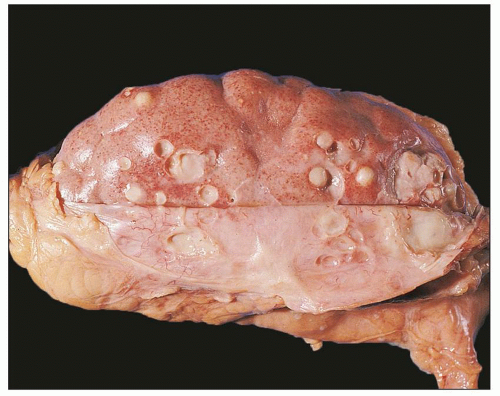 FIGURE 24.9 Diffuse suppurative nephritis. The subcapsular surface shows numerous discrete and focally confluent, whitish-yellow abscesses of variable size. |
to hematogenously spread infection to the kidney. For example, the case shown in Figure 24.11 is from a 68-year-old man with history of weight loss, fatigue, weakness for 2 years, history of colon cancer, and documented blood infection. The glomeruli are filled with periodic acid-Schiff (PAS)-positive rod-shaped Tropheryma whippeli bacteria, better seen by electron microscopy (Fig. 24.12). Acute pyelonephritis was evident in the surrounding renal parenchyma, but the glomeruli are devoid of inflammation in spite of the presence of bacteria.
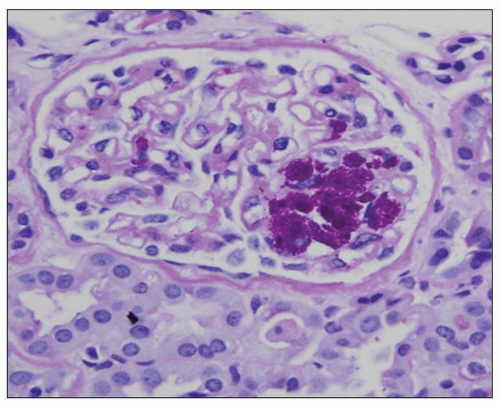 FIGURE 24.11 Acute pyelonephritis from an immunocompromised patient with Tropheryma whippeli infection. PAS-positive organisms are found within the glomerular tuft. (PAS; ×400.) |
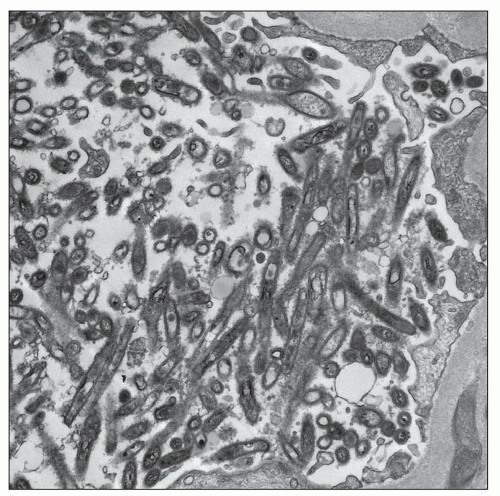 FIGURE 24.12 Transmission electron micrograph demonstrates the rod-like Tropheryma whippeli organisms within the glomerulus. (Courtesy of Carrie Phillips, Indiana University School of Medicine, Indiana.) |
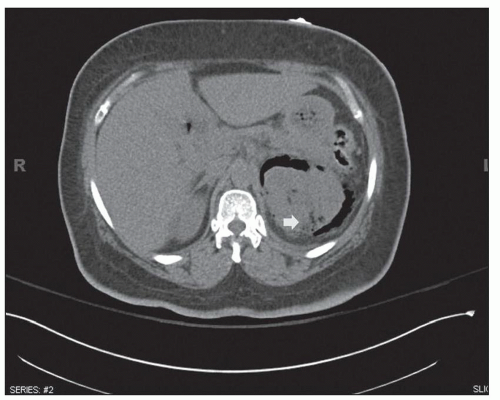 FIGURE 24.13 Emphysematous pyelonephritis. The patient was a 58-year-old woman with history of diabetes who presented with flank pain. CT coronal reconstruction shows gas in the parenchyma of the left kidney and extensive perinephric gas (arrow). (Courtesy of Sanjeev Bhalla, Mallinckrodt Institute of Radiology, Washington University School of Medicine, St. Louis, MO.) |
neurogenic bladder, alcoholism, and anatomic anomalies have also been found in association with this disease (43). Women are affected more often than are men, with a mean age in the sixth decade. Typically, only one kidney is involved, usually the left (3). Rarely, both kidneys are affected (3). Emphysematous pyelonephritis is associated with a 21% mortality rate (44). Patients may have nonspecific clinical symptoms including chills, fever, flank pain, nausea, vomiting, abdominal pain, and pyuria. Patients may initially present with thrombocytopenia, acute renal failure, disturbance of consciousness, and shock, which are risk factors for poor outcome and mortality (44). Escherichia coli is the most common organism encountered, but others, such as Klebsiella pneumoniae, Enterobacter spp., Proteus mirabilis, Candida spp., and Cryptococcus neoformans, have been described. Diagnosis can be made by CT, which also provides information for classifying the extent of the intrarenal and extrarenal disease, which has prognostic and therapeutic importance (2,3,26,27,44). Emphysematous pyelonephritis is a very serious condition that requires prompt and energetic treatment. Operative and nonoperative treatment with antibiotics is currently employed avoiding nephrectomy. The allograft kidney is rarely affected with only about 20 cases of emphysematous pyelonephritis reported in the literature (43). A new radiologic classification is proposed taking into account the extent of gas accumulation in the kidney (class 1 to 4) to help guide appropriate and timely management of patients (44). The pathogenesis of the condition is not clear, but many features are similar to those described in S. aureus infection, suggesting a blood-borne infectious etiology. Four factors involved in pathogenesis include gas-forming bacteria, high tissue glucose, impaired tissue perfusion, and a defective immune response (44,45,62). Successful medical therapy is possible in some cases (45).
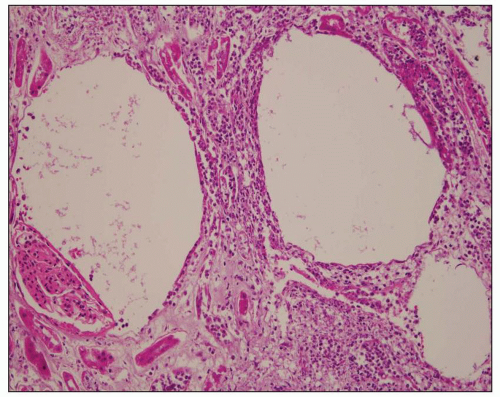 FIGURE 24.14 Emphysematous pyelonephritis. The patient was a 68-year-old diabetic woman. Gas formation in necrotic tissue produces circular spaces resembling pulmonary emphysema. (H&E; ×200.) |
dilated as are all the calyceal systems. The pelvic wall is thickened and granular and often shows signs of congestion owing to active infection. Some cases are associated with stones, typically found in the pelvis and calyces. As a consequence of generalized dilatation of the collecting system, it is common to find a thinned parenchyma, particularly in areas aligned with dilated calyces (Fig. 24.17B). Blunting of the papillae is almost invariably a feature. In some cases, large, discrete scars are seen, as in kidneys with the back-pressure type of reflux nephropathy. Often, however, scars are not apparent, and parenchymal thinning is uniform.
 FIGURE 24.15 Chronic pyelonephritis in an 8-year-old girl with left duplicated ureter and multiple recurrent UTIs, but no evidence of renal dysplasia. The kidney is atrophic with thin cortex and dilated pelvis. The contralateral kidney was intact. |
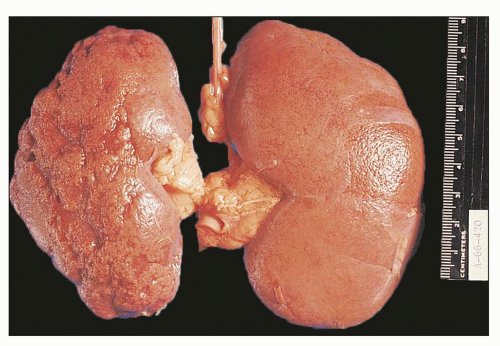 FIGURE 24.16 Chronic pyelonephritis in an adult. Irregular, coarse, depressed scars on the cortical surface of the left kidney are easily appreciated with the capsule stripped. |
calyces, the parenchyma also contains foci of yellowish material. In cases with significant pelvicalyceal dilatation, there may be considerable cortical thinning.
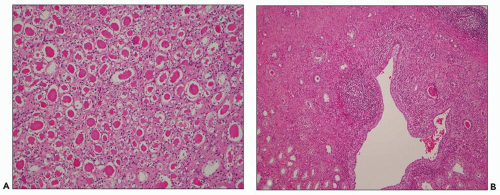 FIGURE 24.17 Chronic pyelonephritis. A: Tubule thyroidization composed of atrophic or dilated tubules with flattened epithelium containing eosinophilic, waxy casts. B: The cortex is thin above the dilated calyx. Lymphoid follicles in the cortex and in the pericalicial region, tubular atrophy and pericalicial fibrosis are present. (H&E; ×100.) |
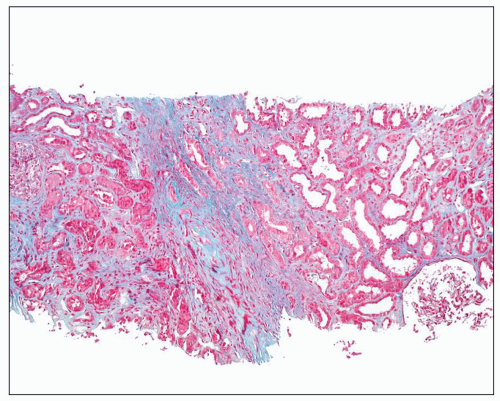 FIGURE 24.18 Chronic pyelonephritis in a 55-year-old man with creatinine of 15 mg/dL secondary to bilateral ureteral obstruction. Renal biopsy was performed to assess extend of damage. Sections show diffuse interstitial fibrosis in a stripped pattern, more pronounced around the collecting ducts. (trichrome stain × 200.) |
 FIGURE 24.19 Xanthogranulomatous pyelonephritis. Contrast-enhanced CT scan demonstrates left kidney enlargement and distension of the collecting system by hypoattenuated material corresponding to inflammatory debris. |
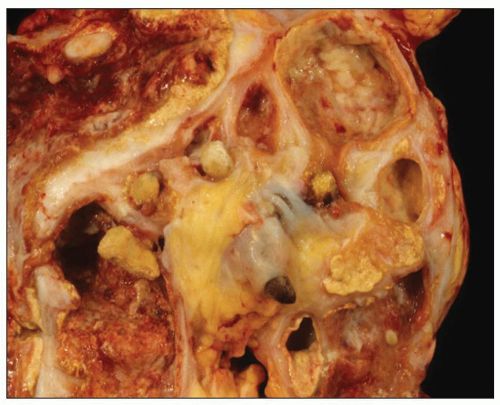 FIGURE 24.20 Xanthogranulomatous pyelonephritis. Friable, yellow tissue surrounds the dilated calyces. Numerous calculi are evident. |
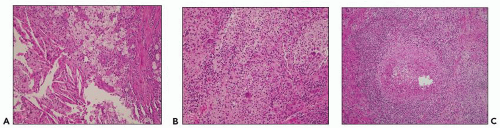 FIGURE 24.21 Xanthogranulomatous pyelonephritis. A: Foamy cells, cholesterol crystals, and granular macrophages. B: Giant cells, mononuclear inflammatory cells, and (C) necrotizing granulomas are characteristic. (H&E; ×400.) |
follow-up analyzed in the review by Tam et al., six developed significant renal impairment with three requiring renal replacement therapy.
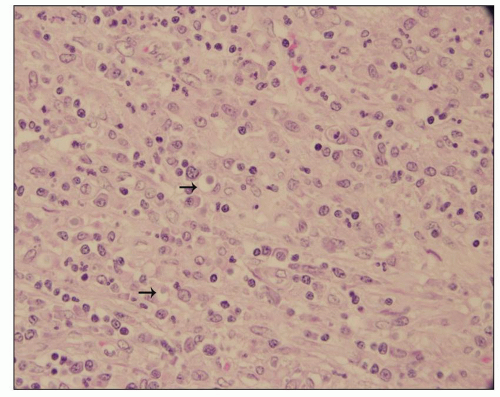 FIGURE 24.22 Malakoplakia. Tubules are destroyed by an interstitial inflammatory infiltrate composed of histiocytes. Numerous intracytoplasmic Michaelis-Gutmann bodies are shown (arrows). (H&E; ×200.) |
PAS. In contrast to malakoplakia, Michaelis-Gutmann bodies are conspicuously absent (63). Given the striking similarities to malakoplakia, it has been proposed that megalocytic interstitial nephritis is a prediagnostic phase of malakoplakia. The differential diagnosis of all entities above includes malignancy, particularly if the lesion is solitary.
TABLE 24.2 UTI pathogenesis: key facts | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
UTIs, especially with regard to renal involvement. The receptorbinding adhesin at the tip of P fimbriae is pap G. There are three classes of G-tip proteins (87). Class II-tip adhesin is associated with pyelonephritis and class III-tip adhesin with cystitis.
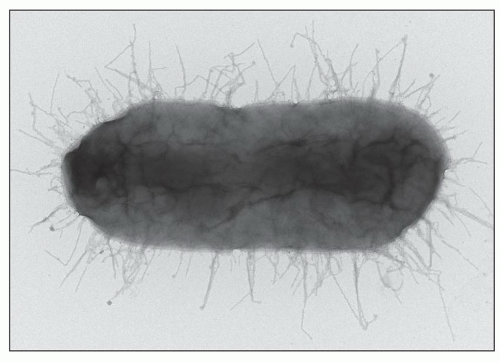 FIGURE 24.23 Uropathogenic E. coli bind to urinary epithelium with fimbriae (pili). P fimbriae (for pyelonephritis-associated pili) are important virulent factors; only bacteria featuring P pili cause pyelonephritis. (electron microscopy-negative stain × 20,000). (Courtesy of Scott Hultgren, Washington University School of Medicine, St. Louis, MO.) |
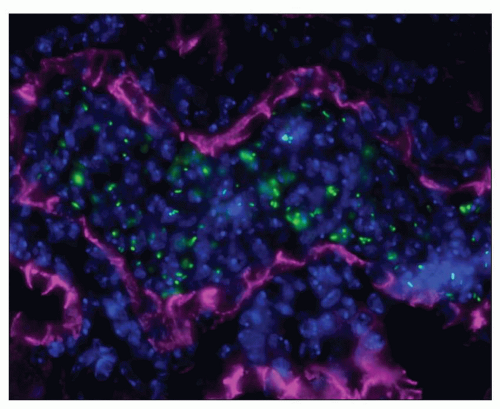 FIGURE 24.24 Experimental pyelonephritis: uropathogenic E. coli (green FITC) induce influx of neutrophils (Hoechst nuclear blue) in tubules (labeled pink with E-cadherin). Mouse kidney immunofluorescence × 63. (Courtesy of Indira Mysorekar, Washington University School of Medicine, St. Louis, MO.) |
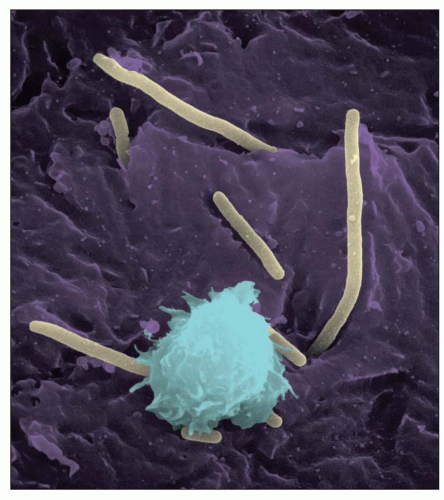 FIGURE 24.25 Scanning EM of urothelial mucosa with adherent bacteria reveals uropathogenic E. coli adhering to and colonizing the urinary bladder (magenta). Inflammatory cells (light blue) are recruited to contain bacterial invasion (pale yellow). (Courtesy of Chia Hung and Scott Hultgren, Washington University School of Medicine, St. Louis, MO.) |
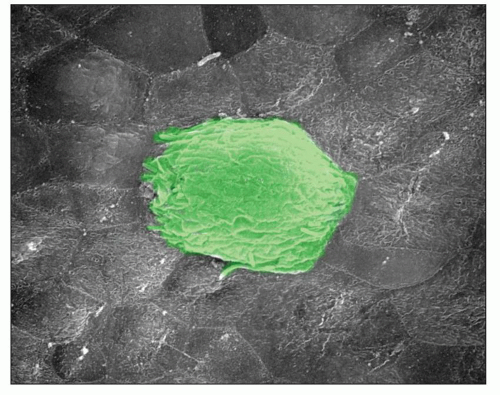 FIGURE 24.26 Scanning EM of an intracellular bacterial community (IBC) on the urothelial surface. Escherichia coli shelter from host defenses leading to persistent bacterial residence within the bladder epithelium. IBCs never form in the kidney; only form in the urinary bladder. Exfoliation of the superficial urothelial layer acts to reduce the bacterial load but facilitates chronic residence of small nests of bacteria that later reemerge to cause recurrent cystitis. (Courtesy of Indira Mysorekar.) |
caseous necrosis (Fig. 24.28). Organisms are usually found in such lesions. Often, a mononuclear infiltrate of lymphocytes, monocytes, and plasma cells is also present. The tubercle may be contained and heal, or the infection may expand. If the medulla is involved, the infection may reach the renal pelvis, allowing release of microorganisms into the urinary tract.
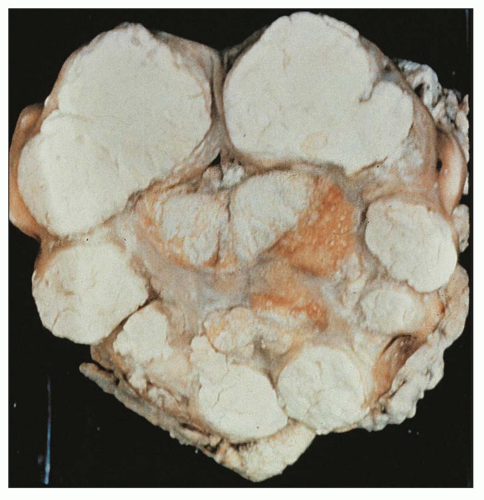 FIGURE 24.27 Tuberculous pyonephrosis. Kidney is filled with cheesy material. |
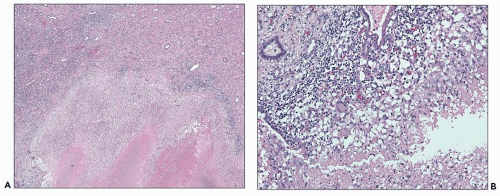 FIGURE 24.28 A: Caseating granulomas with central necrosis and epithelioid histiocytes at the periphery. B: Giant cells are appreciated. (H&E; A, ×100; B, ×400.) (Courtesy of Neeraja Kambham, Stanford University, California.) |
variable interstitial inflammation with lymphocytes and plasma cells amidst calcific foci, probably representing calcified tubercles.
is rare (136). In tissue sections, pseudohyphae and rounded yeast forms, 2 to 4 µm in diameter, predominate (Fig. 24.30). Although Candida can be seen in sections stained with hematoxylin and eosin, they are more readily identified with PAS or Grocott methenamine silver stains.
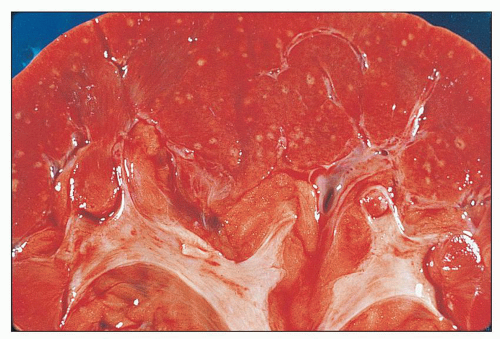 FIGURE 24.29 Candida septicopyemia with scattered small, yellowwhite miliary abscesses. |
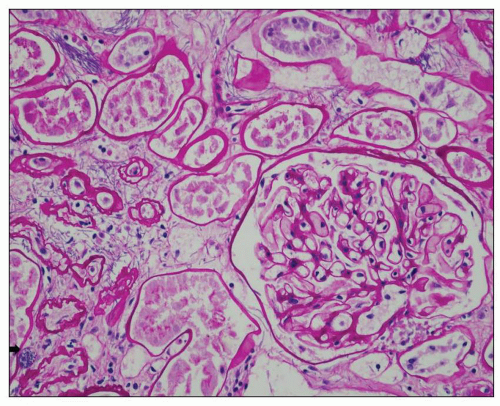 FIGURE 24.30 Renal candidiasis. Bundles of fungal pseudohyphae invade the interstitium and tubules; fungal spores are focally present (arrow); an inflammatory response is lacking. Autopsy kidney from a 49-year-old man who died abruptly from disseminated candidiasis involving multiple organs. (PAS; ×400.) |
tract and mucosal surfaces, cutaneous wounds, or intravenous access lines. Renal aspergillosis is frequently the result of hematogenous dissemination, usually from invasive bronchial infection, necrotizing pneumonitis, or infarct by aspergilli. Patients receiving corticosteroids, neutropenic patients, diabetics, and immunocompromised patients (26) are particularly at risk. Less frequently, the kidneys may be involved through the ascending route (141). Renal parenchymal infections may produce symptoms comparable to those of acute pyelonephritis. The urinary tract may be obstructed by growth of mycelium, and fungus balls may be passed into the urine.
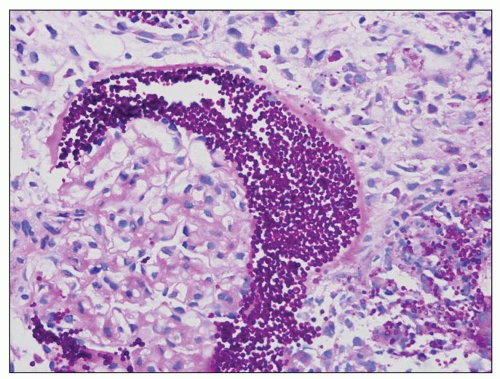 FIGURE 24.31 Renal allograft biopsy from a 50-year-old woman with end-stage kidney disease secondary to diabetes who presented with acute renal failure. Sections show PAS-positive yeast spores in Bowman space and the interstitium. Culture results indicated Candida glabrata. (Courtesy of Salinas-Madrigal, Saint Louis University, St Louis, MO.) |
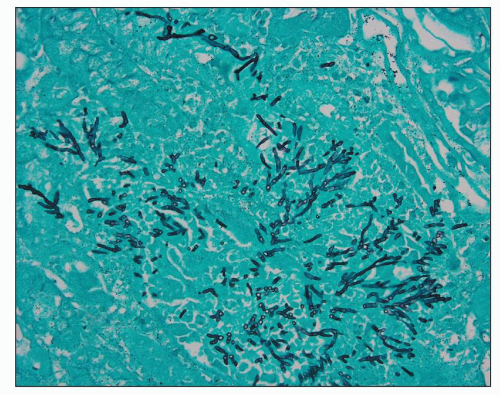 FIGURE 24.32 Renal aspergillosis. Large numbers of branching septate hyphae are illustrated. (methenamine silver × 380.) |
immunosuppression. The disease is not contagious. Renal involvement is usually clinically silent, and compromise of renal function is uncommon.
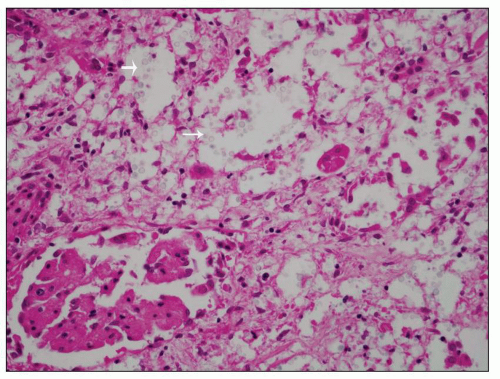 FIGURE 24.33 Renal involvement in systemic cryptococcosis. Yeast within glomeruli and tubules are separated by clear halos corresponding to their thick capsule. (H&E; ×200.) |
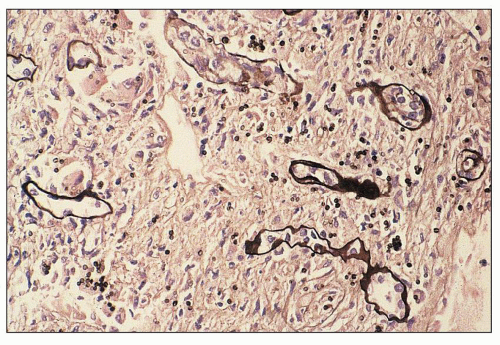 FIGURE 24.34 Histoplasmosis in a renal allograft. Yeast forms of H. capsulatum are highlighted with silver stain (arrows). (methenamine silver × 400.) |
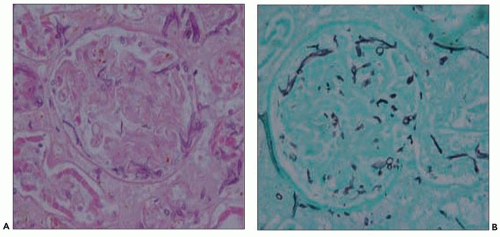 FIGURE 24.35 Renal mucormycosis involving glomeruli. A: Hyphae are broad and nonseptate with right-angle branching. (H&E; ×400.) B: Methenamine silver × 400. (Courtesy of Antony Chang University of Chicago, Chicago, Illinois.) |
encoded molecules and facilitate a TH1 response at the locale of the renal parenchyma. The subsequent inflammatory response may injure the kidney. As a phenotypic disease example of virally induced innocent bystander damage, the hemophagocytic syndrome (HPS), in which nonmalignant proliferations of activated macrophages infiltrate many organs, can cause acute renal failure. Viral triggers such as Epstein-Barr virus (EBV), parvovirus, and CMV have been described in HPS. Heterologous immunity, in which established memory T-cell responses to a previously encountered pathogen, can have a major impact on the course and outcome of a subsequent infection with an unrelated pathogen. Heterologous immunity is dependent on the sequence of infections, the prior T memory network at the time of the infection, and can be either beneficial or detrimental to the host in transplantation settings (149).
of small lymphoid cells, plasma cells, and rare immunoblasts (Fig. 24.36). In “polymorphous PTLD,” the mixed morphotype of the infectious mononucleosis-type reaction is repeated but with a greater number of immunoblasts, occasional atypical immunoblasts, cells with irregular nuclei resembling centrocytes, increased mitoses, and frequently, necrosis (Fig. 24.37). PTLD involving renal allografts does not show the lymphocytic tubulitis or vasculitis of cellular rejection.
TABLE 24.3 World Health Organization categories of PTLD | |||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||
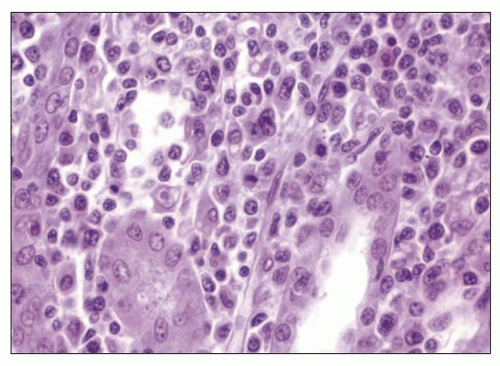 FIGURE 24.36 Early mononucleosis-like infiltrate of PTLD. The interstitial infiltrate is mostly mature lymphocytes. Only rare immunoblasts are seen. (H&E; ×27.) |
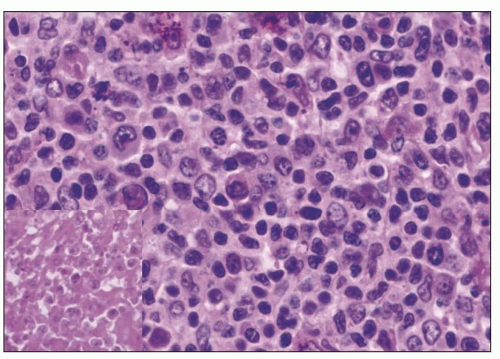 FIGURE 24.37 Polymorphous PTLD. The number of transformed cells is increased, with many immunoblasts. Focal necrosis is seen (inset). (H&E; ×27.) |
for PTLD, including studies for EBV and C4d, should be undertaken in renal allograft recipients with dense lymphoid infiltrates showing atypia and/or interstitial hemorrhage.
adenovirus are well described in immunosuppressed patients including solid organ and bone marrow transplant patients and may present as disseminated infection (180). Adenovirus infection may also present as acute hemorrhagic cystitis in renal transplant patients (181). Adenovirus viremia is cited in approximately 7% of renal transplant patients (182), and the virus is excreted in approximately 11% (183). Serotypes 7, 11, 34, and 35 constitute most of the cases (184). Adenovirus has tropism for epithelial cells via coxsackievirus and AdV receptors, class I human leukocyte antigen molecules, and sialoglycoprotein receptors (185); CD46; and fiber knob gene protein (186). Secondary interactions with integrins may be needed for virus internalization.
Related posts:
 Development of the Kidney
Development of the Kidney
 Membranous Glomerulonephritis
Membranous Glomerulonephritis
 IgA Nephropathy and IgA Vasculitis (Henoch-Schönlein Purpura) Nephritis
IgA Nephropathy and IgA Vasculitis (Henoch-Schönlein Purpura) Nephritis
 Renal Involvement in Polyarteritis Nodosa, Kawasaki Disease, Takayasu Arteritis, and Giant Cell Arteritis
Renal Involvement in Polyarteritis Nodosa, Kawasaki Disease, Takayasu Arteritis, and Giant Cell Arteritis
 Glomerular Diseases With Organized Deposits
Glomerular Diseases With Organized Deposits
 Renal Changes With Aging and End-Stage Renal Disease
Renal Changes With Aging and End-Stage Renal Disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


