Chapter 42 THE SPARC SLING SYSTEM
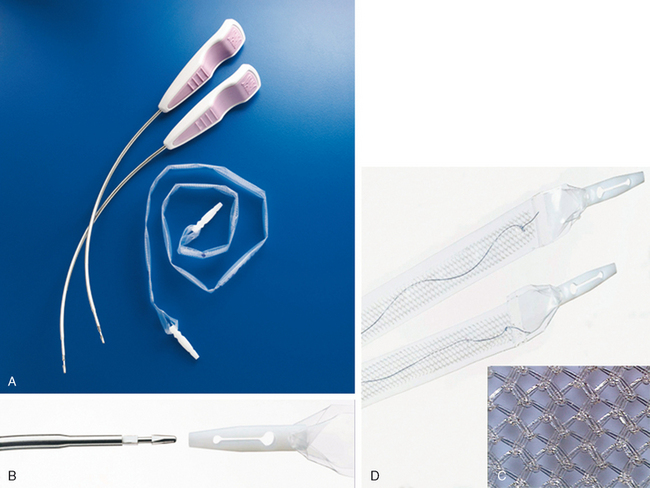
The SPARC Sling System (American Medical Systems, Minnetonka, MN) is a minimally invasive pubovaginal sling procedure using a loosely knitted, self-fixating, 1-cm wide, 4-0 polypropylene mesh, which is placed at the level of the mid-urethra by passing the suspension needle via a suprapubic-to-vaginal approach.1–3 The placement of pubovaginal slings in the treatment of genuine stress urinary incontinence has historically been effective, with excellent long-term outcomes.4 This variation of surgical technique results from the drive to decrease surgical morbidity associated with autologous fascia harvesting; it also minimizes the risk of intraoperative complications from minimally invasive sling placement without affecting surgical outcomes (Fig. 42-1).5–12
MECHANISM OF ACTION
Continence results from multiple factors: resting urethral tone, active sphincter contraction, external compression, pressure transmission, and integrity of anatomic configuration. The success of midurethral sling techniques has prompted a reevaluation of the pathophysiology of genuine stress urinary incontinence and the paradigm for its surgical correction. The mechanism of action for midurethral slings is presumed to be mimicking of the support provided by the pubourethral ligaments and suburethral fascial support.13
The importance of urethral stabilization from rotational motion has generally been accepted and was introduced as the “integral theory” based on data collected during radiologic evaluation of micturition.14 This correlated with structures documented on anatomic dissection and was dubbed an “anatomic hammock.”15 The importance of urethral configuration suggests that midurethral support prevents separation of the posterior urethral wall from the anterior urethral wall during rotational motion around the inferior portion of the pubic ramus, which appears integral to continence.16 Suburethral support and stability, in conjunction with urethral coaptation, appears to be the critical factor in the restoration of continence, and elevation of the bladder neck may no longer be a prerequisite.
SURGICAL TECHNIQUE
Incisions
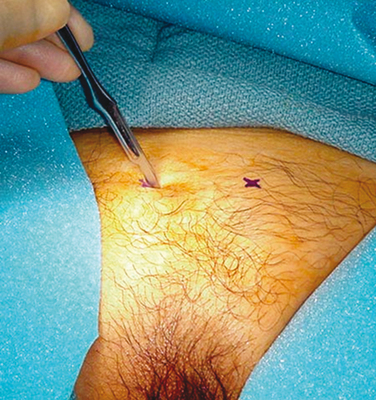
Two parallel, 15-blade stab incisions are made above the pubic symphysis 1.5 cm from the midline (3 cm apart). The surgeon should avoid incisions lateral to this area to keep away from the ilioinguinal nerve exiting from the external ring (Fig. 42-2).
Next, the bladder neck should be identified, the submeatal fold may be elevated using an Allis clamp, and a midline incision is performed through the vaginal mucosa over the mid-urethra. This incision, centered over the mid-urethra, may vary between 1.5 and 3 cm (Fig. 42-3). If the procedure is performed without local anesthetic, a saline injection at the level of the mid-urethra, extending laterally, may be elected to aid in development of the plane of dissection between the vaginal epithelium and the periurethral fascia. Metzenbaum scissors are used to create a submucosal tunnel to the inferior border of the pubic ramus at the level of the mid-urethra bilaterally. The tunnels may be narrow enough for just the needle and connector dilator to traverse the distance, or they may be wide enough to accommodate insertion of a fingertip. With the “narrow tunnel” approach, the fingertip is placed in the paravaginal fornix, outside the incision, in order to palpate needle perforation through the endopelvic fascia (recommended).

Needle Passage
Related posts:
 DEVELOPMENTAL ANATOMY AND UROGENITAL ABNORMALITIES
DEVELOPMENTAL ANATOMY AND UROGENITAL ABNORMALITIES
 USE OF CADAVERIC FASCIA FOR PUBOVAGINAL SLINGS
USE OF CADAVERIC FASCIA FOR PUBOVAGINAL SLINGS
 EPIDEMIOLOGY OF INCONTINENCE AND VOIDING DYSFUNCTION IN THE ELDERLY
EPIDEMIOLOGY OF INCONTINENCE AND VOIDING DYSFUNCTION IN THE ELDERLY
 SURGERY FOR REFRACTORY URINARY INCONTINENCE: SPIRAL SLING
SURGERY FOR REFRACTORY URINARY INCONTINENCE: SPIRAL SLING
 FEMALE SEXUAL FUNCTION AND DYSFUNCTION
FEMALE SEXUAL FUNCTION AND DYSFUNCTION
 FUNCTIONAL ANATOMY AND PATHOPHYSIOLOGY OF PELVIC ORGAN PROLAPSE
FUNCTIONAL ANATOMY AND PATHOPHYSIOLOGY OF PELVIC ORGAN PROLAPSE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


