Chapter 93 EPIDEMIOLOGY OF INCONTINENCE AND VOIDING DYSFUNCTION IN THE ELDERLY
The understanding of epidemiology—the study of the distribution and determinants of disease—is critical in the search for the risk and protective factors that lead to primary or secondary disease prevention. This is especially true of urinary incontinence and voiding dysfunction, conditions that are multifactorial in origin. Although there is still a major gap in our knowledge about the issues involved in the epidemiology of these conditions, there has been a significant advance in the procurement of epidemiologic information in many parts of the world. This new-found enthusiasm led to the to the realization that urinary incontinence and voiding dysfunction are highly prevalent and that the consequences can be devastating for the afflicted women and have a tremendous impact on the nation’s health care system. Largely because of these research initiatives, treatment and preventive strategies have emerged.
URINARY INCONTINENCE
The International Continence Society defines incontinence as “the complaint of any involuntary leakage of urine.”1 The prevalence of urinary incontinence is defined as the probability of incontinence within a defined population group within a specified time period. The concept is important for establishing the distribution of the condition in the population and for projecting the need for health and medical services. The prevalence of all cases of urinary incontinence is estimated as the ratio of the number of incontinence respondents identified in a cross-sectional survey of continent and incontinent subjects. The prevalence of specific types and severity levels is estimated in an analogous manner. Any studies on the epidemiology of incontinence and voiding dysfunction or any condition or disease depend significantly on the definition of the condition and on the method used to obtain the information. The lack of a uniform definition of urinary incontinence is a fundamental problem in assessing and comparing the findings in different studies.
Prevalence of Urinary Incontinence in the Community
The pioneering studies on the prevalence of incontinence were done in Europe and mainly included subjects living in the community. From these early investigations, it was established that urinary incontinence is much more prevalent among the elderly than in any other age group living in the community. The sentinel paper published in 19682 was followed by a comprehensive study by Thomas and colleagues3 in 1980. The group carried out a postal survey of two London boroughs and assessed 22,430 female subjects 5 years old or older. The survey team defined regular incontinence as two or more episodes of urinary incontinence occurring in the past month, whereas occasional incontinence was defined as less than two incontinence episodes per month. The group reported the prevalence of incontinence in all age groups (5 to more than 85 years) to be 8.5%. The prevalence rates of urinary incontinence in the different age groups are shown in Table 93-1.
Table 93-1 Prevalence of Urinary Incontinence in Women Living in London
| Age Group (Years) | Regular Urinary Incontinence (%) | Occasional Urinary Incontinence (%) |
|---|---|---|
| 5-14 | 5.1 | 11.2 |
| 15-24 | 4.0 | 11.9 |
| 25-34 | 5.5 | 20.0 |
| 35-44 | 10.2 | 20.7 |
| 45-54 | 11.8 | 21.9 |
| 55-64 | 11.9 | 18.6 |
| 65-74 | 8.8 | 14.6 |
| 75-84 | 16.0 | 13.6 |
| ≥85 | 16.2 | 16.2 |
| Total | 16.6 | 8.5 |
From Thomas TM, Plymat KR, Blannin J, et al: Prevalence of urinary incontinence. BMJ 281:1243, 1980.
When incontinence was correlated with previous pregnancy and with the number of pregnancies, nulliparous women were found to have a lower prevalence than those who had one or more babies. The number of pregnancies did not make any difference among the incontinent respondents, except those in the 45- to 54-year age group, in which those who had had four or more babies were most likely to report regular incontinence. Incontinence was also reported to be moderate or severe in approximately 20% of the respondents, of whom less than one third received health or social services for the condition.
A European epidemiologic study was conducted by Hunskaar and coworkers4 in four countries. Based on a mail survey of 29,000 households representing the general population of adult women 18 years or older (mean, 46.3 years) and on incontinence defined as any leakage or involuntary loss of urine during the preceding 30 days, the group reported the prevalence of incontinence to be 15% for women in Spain, 32% in France, 32% in the United Kingdom, and 34% in Germany. The survey also determined the type of incontinence. Stress urinary incontinence symptoms were defined as a leak or loss of urine caused by sneezing, coughing, exercising, lifting, or physical activity. Urge urinary incontinence symptoms were defined as an urge to urinate but being unable to reach the toilet before leaking or having a strong sudden urge to go to the toilet to urinate with no advance warning. Mixed urinary incontinence symptoms were defined as at least one stress and one urge symptom. Among the adult women in four countries, stress (37%) and mixed (33%) types were shown to be more predominant than urge incontinence (20%) and other (10%) types. In the subpopulation of women 60 years old or older, the mixed type predominates (41%), followed by stress incontinence (31%), urge incontinence (22%), and other types (6%).
The prevalence of any type of urinary incontinence by age shows an intriguing pattern. A survey of Norwegian women 20 years old or older found a gradual increase of prevalence across adulthood until age 50, when the prevalence reaches 30%, and then a stabilization or even slight decrease until age 70, when prevalence starts increasing again. The severity of incontinence also increases regardless of the type of incontinence with advancing age (Fig. 93-1).5
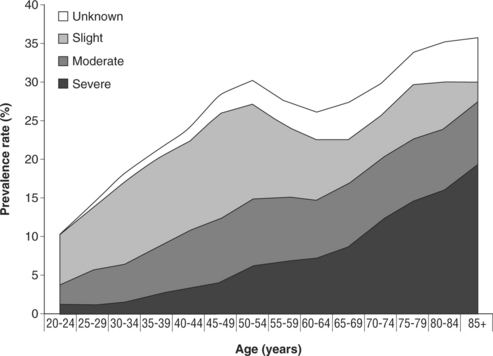
Figure 93-1 Prevalence of urinary incontinence by age group and severity in the Norwegian EPINCONT study.
(From Hannestad YS, Rortveit G, Sandvik H, et al: A community-based epidemiological survey of female urinary incontinence: The Norwegian EPINCONT study. J Clin Epidemiol 53:1150-1157, 2000.)
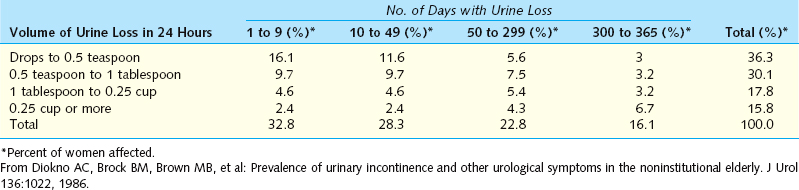
In the United States, the first comprehensive epidemiologic study on urinary incontinence in the elderly living in the community was the Medical Epidemiologic and Social Aspect of Aging (MESA) survey, which was conducted in 1983 in Washtenaw County, Michigan, by Diokno and colleagues.6 This was a cross-sectional and longitudinal study of elderly respondents 60 years old or older sponsored by National Institute of Aging. A multistage stratified area probability sample of the Washtenaw County identified 13,912 households that were screened by household interviewers to identify households containing one or more persons 60 years old or older. The prevalence of urinary incontinence among all women 60 years old or older interviewed was 38%. The severity of urinary incontinence was analyzed according to the quantity of urine loss per day and the frequency of urine loss in 365 days (Table 93-2). The clinical type of urinary incontinence was also detailed in the MESA study. The result showed the mixed type of incontinence was the most prevalent, involving 55% of the incontinent responders, followed by stress (27%), urge (9%), and the other category (9%).
Table 93-2 Severity of Urinary Incontinence by Volume and Frequency of Urine Loss in Women 60 Years or Older
A more recent epidemiologic study in the United States was reported by Kinchen and associates7 in 2002. The team conducted a national, cross-sectional, mailed survey of 45,000 households to determine the prevalence of urinary incontinence in adult women 18 years old or older. Among the 24,443 female respondents, 37% reported urinary incontinence in the past 30 days. The type of incontinence also depicts a higher prevalence rate for mixed (45%) and stress (41%) incontinence than for urge incontinence (12%). Age of onset differs by the type of incontinence. The median age of women was 48 years old for those reporting stress incontinence, 55 years for mixed incontinence, and 61 years for urge incontinence.7
In Asia, an epidemiologic study (cross-sectional, mailed survey) was done by the Asian Society for Female Urology (ASFU) to determine prevalence of overactive bladder symptoms and incontinence in 11 Asian countries.8 The questionnaire used to establish the prevalence of incontinence, however, was different from the American and European surveys in that it was more focused on urge incontinence than on any type of incontinence. The prevalence of urinary incontinence ranged from 17% for Thailand and 13% for the Philippines to 4% for Singapore and China. The Asian survey also reported a much higher prevalence of mixed incontinence of 64%, with urge incontinence at 23% and stress incontinence at 13%.
Prevalence of Urinary Incontinence in Institutions
The prevalence of urinary incontinence is much higher among institutionalized women. A survey sponsored by the United States Department of Health, Education, and Welfare about long-term facilities reported that 55% of patients surveyed had some problems with urinary control and that an additional 5% of patients were using a catheter or some collecting device.9 Similarly, the National Nursing Home Survey sponsored by the National Center for Health Statistics confirmed the prevalence of incontinence of 50% among the more than 1.5 million nursing home facility residents in the United States.10 Willington11 estimated that 30% of unselected elderly admissions have urinary incontinence.
Some studies suggest institutional prevalence ranges between 6% and 72%.12 Several reviews from around the world, some of which sample of institutions rather than individual institutions, suggests a prevalence of 50% or higher.13–20 The range of prevalence in institutions is probably a consequence of the definition of urinary incontinence and criteria for admission to residential care, which vary within countries and among facilities.21 The process that results in the relatively high prevalence of urinary incontinence in residential care facilities remains unclear. Thom and colleagues22 reported that the relative risk of admission to a nursing home was two times greater for incontinent women after adjustments for age, cohort factors, and comorbid conditions. These findings suggest that incontinence may contribute to institutionalization. However, an alternative explanation of residential care contributing in some way to the development of incontinence cannot be excluded with confidence.
Racial and Ethnic Differences
Most epidemiologic studies of urinary incontinence have been conducted on white populations. The data available on black women indicate that they are less susceptible to urinary incontinence than white women.23 However, in those who were incontinent, the severity was not significantly different between the two racial groups.23,24
It was suggested that black and white women have different factors promoting urinary incontinence.25 The clinical data in the United States indicate that black women have higher urethral closure pressure, larger urethral volume, and greater vesical mobility compared with white women.26 This difference in physiologic subtypes was supported by data confirming a significant difference in the predominance of stress incontinence in white women.27 Black South African women rarely develop stress incontinence and the related disorder of pelvic floor prolapse, at a rate 80 times lower than whites.28 Later studies later attempted to explain these observations as a function of different urethral pressures and lengths and pubococcygeal muscle strength.29,30
The prevalence of urinary incontinence among the Hispanic women 65 years old or older in the United States is lower than the general population. Using a methodology similar to the MESA study, Espino and coworkers31 reported a prevalence rate of 15%. Similarly, mixed incontinence predominates at a rate of 42%, urge at 33%, and stress incontinence at 10%.
Incidence and Remission Rates
The incidence of urinary incontinence is the probability of becoming incontinent during a defined period of time. The concept is helpful in determining the onset and in understanding the risk factors for the condition. There are few epidemiologic data on the development or natural history of urinary incontinence and its transition to various levels of severity and type of incontinence. Campbell and associates32 reported an incidence rate of incontinence among women 65 years old or older in New Zealand to be about 10% in a 3-year period. Moller and colleagues33 and Samuelsson and coworkers34 reported an incidence of 6% and 3% in young and middle-aged women, respectively. During the 5-year follow-up, the annual incidence was 2.9%, with severe incontinence at occurring at a rate of 0.5%. The remission rate (i.e., women who were incontinent at baseline and became incontinent at the end of study) was 5.9%.
In the MESA survey, the incidence of elderly women who were continent at the initial baseline interview and became incontinent a year later (i.e., second interview) was 22.4%. The incidence at the third interview of respondents who were still continent during the second interview was 20.2%. The remission rate during the second interview was 11.2%. Similarly, 13.3% of the incontinent respondents at the second interview became continent by the third interview. When a continent woman becomes incontinent the subsequent year, the most likely pattern is a mild form of incontinence. About one half of the cases of mild incontinence at the beginning of survey remained mild; few became severe. Women with severe incontinence usually remained severely incontinent after 1 year of follow-up. One half of the cases of moderate incontinence remained moderate, and the rest became mild or severe. In terms of the type of incontinence, women who originally had stress incontinence remained the same or developed the mixed type. Women with the mixed type usually stayed the same. Most continent women who became incontinent developed the stress type or a mixed stress-urge type of incontinence.
The current interpretation of the data indicates that the substantial incidence rates are paralleled by equally substantial remission rates. However, it is not clear whether the level of remission reflects active treatment or intervention or it is part of the natural course of incontinence.35
Correlates of Urinary Incontinence
Urinary incontinence is a condition of multifactorial origin. The MESA study investigated and reported the many suspected correlates of incontinence. The factors investigated extended beyond the medical correlates into social and psychological aspects. Among women, the measures of depression, negative affect balance, and life satisfaction reflect to a statistically significant degree the effect of incontinence.36 Continent older women reported the highest levels of psychological well-being (i.e., the least depression and negative affect balance) and the most life satisfaction. Psychological well-being declines with increasing severity of urinary incontinence; the more severely incontinent women experience higher depression and negative affect balance and lower life satisfaction than the less severely incontinent women or continent women. Changes in the measures of happiness and positive affect balance are not as clear. Herzog and colleagues37 suggested that these relationships are partly explained by the fact that incontinent respondents are less healthy than the continent respondents.
Related posts:
 DEVELOPMENTAL ANATOMY AND UROGENITAL ABNORMALITIES
DEVELOPMENTAL ANATOMY AND UROGENITAL ABNORMALITIES
 USE OF CADAVERIC FASCIA FOR PUBOVAGINAL SLINGS
USE OF CADAVERIC FASCIA FOR PUBOVAGINAL SLINGS
 ANTERIOR COLPORRHAPHY FOR CYSTOCELE REPAIR
ANTERIOR COLPORRHAPHY FOR CYSTOCELE REPAIR
 TRANSVAGINAL CLOSURE OF THE BLADDER NECK IN THE TREATMENT OF URINARY INCONTINENCE
TRANSVAGINAL CLOSURE OF THE BLADDER NECK IN THE TREATMENT OF URINARY INCONTINENCE
 FEMALE SEXUAL FUNCTION AND DYSFUNCTION
FEMALE SEXUAL FUNCTION AND DYSFUNCTION
 FUNCTIONAL ANATOMY AND PATHOPHYSIOLOGY OF PELVIC ORGAN PROLAPSE
FUNCTIONAL ANATOMY AND PATHOPHYSIOLOGY OF PELVIC ORGAN PROLAPSE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


