Renal Artery Thrombosis, Thromboembolism, Aneurysms, Atheroemboli, and Renal Vein Thrombosis
Renal Artery Thrombosis, Thromboembolism, Aneurysms, Atheroemboli, and Renal Vein Thrombosis
John W. O’Bell
George P. Bayliss
Lance D. Dworkin
This chapter focuses on vascular complications of the main renal arteries and veins. The chapter is divided into the following subsections: (1) acute thrombosis of the renal artery from trauma; (2) nontraumatic renal arterial occlusive disease; (3) renal artery aneurysms, including ruptured aneurysm; (4) renal artery dissecting aneurysms; (5) atheroembolic renal disease; and (6) acute and chronic renal vein thrombosis. Because renal vein thrombosis occurs primarily in patients with nephrotic syndrome, particular attention will be paid to the discussion of the hypercoagulability of nephrotic syndrome. Although some of the conditions described may participate in the pathophysiology of renovascular hypertension, they are listed for purposes of a differential diagnosis, as renovascular hypertension is discussed in detail elsewhere.
ACUTE THROMBOSIS OF THE RENAL ARTERY FROM TRAUMA
Blunt abdominal trauma such as that occurring after a motor vehicle accident is the most common cause of renal artery thrombosis.1,2 The mechanism of injury is felt to be acute deceleration injury causing intimal tears, subintimal dissection, and resultant thrombosis.3 Increased mobility of the left kidney and a more acute angle of attachment to the aorta are felt to explain the observation that the left renal artery is more frequently involved than the right3 although in some series this pattern is not observed.4 Injuries to other abdominal viscera are commonly reported due to the severity of the abdominal trauma.3,4,5,6 In a review of 250 cases of traumatic renal artery injury requiring surgical exploration, the following patterns were observed: thrombosis (52%) was the most common finding followed by avulsion (12%), branch injury, and lacerations (3%).6 Bilateral renal artery findings were noted in 9% and injury to other abdominal organs was present 45% of the time.6 Renal artery dissection with resultant thrombosis has also been reported after vigorous exercise such as prolonged cycling,7 marathon running,8 and aerobics.9 Isolated cases of traumatic dissection due to seat belt related injury10 and shock wave lithotripsy11 have also been reported in the literature.
The major concern with renal arterial thrombosis is renal infarction and permanent loss of function. Although the maximal duration of warm ischemia tolerated by human kidneys is uncertain, warm ischemia time as short as 1 to 2 hours may be sufficient to cause irreversible loss of renal function.12 Animal studies have helped further understanding of the importance of even low amounts of blood flow in maintaining renal viability. In dog models of unilateral renal artery occlusion by clamping, warm ischemia times of 1, 2, and 3 hours resulted in irreversible loss of viability in the occluded kidney in 40%, 62%, and 100%, respectively.12,13,14 In contrast, animals subjected to a partial occlusion of the suprarenal aorta (mean arterial pressures downstream of 17 to 30 mm Hg) tolerated up to 2 hours of reduced perfusion with good recovery in all the animals. For these reasons, the extent of occlusion and presence or absence of collateral circulation may have a major impact on viability of the affected kidney.
Clinical Features
Anuria or oliguria are likely to be present in bilateral renal arterial thrombosis, or unilateral thrombosis in patients with a solitary kidney, but are uncommon features in patients with unilateral thrombosis. Laboratory abnormalities may include hematuria, elevations in lactate dehydrogenase (LDH), creatinine kinase (CK), aspartate aminotransferase (AST), and alkaline phosphatase.1 Flank pain or abdominal pain are common, but considering most cases are related to trauma, may not be reliable indicators as there may be alternate explanations for pain.
Diagnosis
Because of the short duration of warm ischemia time that can be tolerated by the kidneys, timely diagnosis is critical. Computed tomography (CT) with intravenous contrast is a useful study in patients with abdominal trauma and compares favorably to angiography, the gold standard for renal artery injury or thrombosis.14 Characteristic CT findings are a lack of renal parenchymal contrast uptake and excretion. The “cortical rim sign” or contrast enhancement of the peripheral renal cortex may be noted and is attributed to collateral or capsular perfusion.15 Angiography remains the gold standard study, and may provide information about collateral circulation (which may indicate better chance for preserved renal viability).16 Use of digital subtraction angiography or imaging with carbon dioxide and/or gadolinium can reduce or eliminate the need for contrast if there are concerns about contrast-induced nephrotoxicity.17 Concerns about exposure to gadolinium and its link to nephrogenic systemic fibrosis in patients with acute or chronic kidney failure may limit its utility in some patients. In patients too unstable for extensive preoperative imaging, even a “one shot” excretory urogram following a bolus injection of contrast may provide useful information to the surgeon as a normal urogram would exclude the presence of major trauma to that kidney. This could be of use in predicting renal outcome in a patient requiring unilateral nephrectomy to control hemorrhage as normal imaging of the contralateral kidney suggests a better outcome.18
Treatment
Treatment for unilateral traumatic renal artery occlusion can be supportive, surgical, or endovascular. Early surgical intervention has been attempted in an effort to salvage renal function, but with mixed results. Factors influencing surgical outcomes include duration of warm ischemia, severity of occlusion (complete or partial), and degree of collateral circulation.18,19,20,21,22,23,24,25 Case series suggest better results with earlier intervention. Maggio and Brosman reported 80% success of renal salvage when revascularization occurred within 12 hours of injury, 57% success for repairs performed between 12 and 18 hours, and 0% for later attempts.25 Clark et al. reported substantially lower success rates despite earlier revascularization attempts (17% success rate for revascularization performed 3-18 hours after the injury).6 Haas et al. reviewed cases from their own institution and from the literature and reported surgical outcomes of 20 cases of bilateral occlusion and 34 cases of unilateral renal arterial occlusion.4,5 In these cases surgical revascularization was successful in 56% of the bilateral cases and 26% of the unilateral cases.
More recently, an endovascular, rather than surgical approach has been attempted in order to salvage renal function. Good outcomes have been reported in isolated cases of traumatic renal artery occlusion following endovascular stenting procedures, in some cases as long as 24 hours following the injury.2,26,27 Even following a successful endovascular procedure, the presence of more peripheral thrombi may still limit recovery of renal function.28 Considering these cases are related to trauma, the decision regarding an endovascular versus a surgical approach may be dictated by the presence of other injuries and need for other abdominal surgery to address those injuries or to control hemorrhage.
In general, surgical or endovascular intervention is reserved for patients with bilateral renal artery occlusion, or unilateral occlusion in patients with a solitary kidney. It is not clear that revascularization of a unilateral occlusion offers advantages over medical management when there is normal function of the contralateral kidney. Although reports in the literature raise significant concerns about viability of the ischemic kidney when thrombosis is prolonged, there are still scattered reports of successful revascularization long after the injury.23,24,25,29,30 Other factors such as collateral circulation or incomplete occlusion may have played a role in some of the reported successes.
In cases of surgical revascularization, it is advised not to perform isolated thrombectomy.4 Resection of the occluded segment with reattachment to the aorta, or placement of an aortorenal graft is advised.29 In surgical cases with substantial hemorrhage, urgent nephrectomy may be required.
NONTRAUMATIC RENAL ARTERY OCCLUSIVE DISEASE
In addition to traumatic injury resulting in renal arterial thrombosis, there are a variety of nontraumatic causes for renal arterial occlusion. These may be related to thromboembolic disease from a cardiac or other source, or thrombotic disease, for example from local endothelial damage such as that seen in atherosclerosis, or systemic hypercoagulable states. A number of causes for nontraumatic renal artery thrombosis are listed in Table 56.1.
Any disease process that disrupts the arterial endothelial surface can cause acute thrombosis. Most common among these is atherosclerotic renovascular disease. Other possible causes include fibromuscular dysplasia,31,32 inflammation/vasculitis, infection, aneurysms, or dissection. Renal arterial thrombosis has been reported in the medium and large vessel vasculitides, including Takayasu arteritis,33,34 polyarteritis nodosum,35,36 and Behçet disease.37,38,39,40 Other unusual causes include syphilis,41 cocaine use,42,43,44 phycomycosis,45,46 neurofibromatosis,47 and urothelial carcinoma of the renal pelvis.48 Sickle cell anemia typically leads to microscopic infarcts and progressive loss of renal function, but large vessel thrombosis with resulting infarction has been reported as well.49 Congenital disorders of collagen structure such as Ehlers-Danlos syndrome are also associated with renal artery thrombosis.50,51
Hypercoagulable states are much more commonly associated with venous thrombosis, including renal vein thrombosis, which is discussed elsewhere in this chapter. Notable exceptions include antiphospholipid antibody syndrome (APS), particularly catastrophic APS, and heparin-induced thrombocytopenia.52 Primary or secondary (lupus-related) APS have been implicated in renal artery thrombosis and reported extensively.56,57,58,59,60,61,62,63 Renal infarct was a common finding in a recent review of abdominal CT scans for patients with APS, occurring in 22 of the 215 patients and accounting for over 50% of the intra-abdominal thromboses.64 Renal arterial thrombosis has also been reported in antithrombin 3 deficiency65 and has been reported rarely in patients with nephrotic syndrome.66,67,68 Factor V Leiden deficiency, again a much more common cause of venous thrombosis, has been associated with renal arterial thrombosis in native and transplanted kidneys.69
TABLE 56.1 Nontraumatic Causes of Acute Occlusive Renovascular Disease
Renal Artery Thrombosis
Endothelial damage
Atherosclerotic disease
Fibromuscular dysplasia
Renal artery aneurysms and dissecting aneurysms
Polyarteritis nodosum
Takayasu arteritis
Kawasaki disease
Thromboangiitis obliterans
Behçet disease
Syphilis
Cocaine
Ehlers-Danlos syndrome
Hypercoagulable state
Antiphospholipid antibody syndrome
Heparin-induced thrombocytopenia
Factor V Leiden mutation
Nephrotic syndrome
Renal Artery Thromboembolism
Cardiac origin
Atrial fibrillation
Endocarditis
Myocardial infarction
Cardiomyopathy
Paradoxical emboli through patent septal defect
Aortic or renal artery source
Severe atherosclerosis/thrombosis
Thromboembolic Disease
Emboli to the renal arteries are typically of cardiac origin. These may be arrhythmia associated, particularly with atrial fibrillation.70,71,72 Mural thrombi as can be seen in acute myocardial infarction or severe cardiomyopathy may also be the source. Thrombi may also occur on diseased or prosthetic heart valves. Septic emboli in the setting of bacterial endocarditis may also be a cause of embolic occlusion and renal infarct, up to 31% in one retrospective series looking at renal biopsy and necropsy results.73 Renal artery embolism may also be seen in cases of atrial or ventricular myxoma.74,75 Paradoxical arterial emboli in the setting of a venous thrombosis and an atrial or ventricular septal defect have also been reported.76 Sources of noncardiac emboli include clots developing elsewhere in arterial circulation and embolizing the renal arteries, or thrombi that originate within aneurysms of the suprarenal aorta or renal artery.
With the advent of increased numbers of endovascular procedures, including angioplasty and stent treatment for aortic and renal artery lesions, iatrogenic causes of renal artery thromboembolism are an increasing concern. Major complications such as thrombosis, dissection, rupture, and atheroembolic showering have been reported to complicate as many as 7% to 10% of endovascular aortic and renovascular procedures.77,78 Morris et al. in 2001 reported renal artery rupture or occlusion from acute thrombosis in 4.2% of 308 renal artery angioplasties with and without stenting.79 In a more recent retrospective analysis of 203 renal artery angioplasty with and without stenting procedures, Eklof et al. reported a rate of distal embolization of 2.5% and renal artery occlusion occurred in only a single patient (0.5%).80 Another concern is the possibility for in-stent thrombus formation in patients following renal artery stenting.81,82 Renal infarction may also occur as a complication of aortic procedures. In two series of 775 thoracic and abdominal aortic aneurysm repairs using a variety of endografts and techniques, the incidence of renal infarction (diagnosed by postprocedure CT scan) was around 10%.83,84 Most were small and asymptomatic, but one of the two series reported a 2.6% incidence of total unilateral renal arterial occlusion.83
A variety of devices have been manufactured to limit the impact of distal emboli following endovascular procedures. Limited studies have demonstrated efficacy in capturing embolic debris,85 but it remains unclear whether such devices will be shown to decrease or prevent distal embolic complications.86 A combination of antiplatelet therapy (abciximab) and distal embolic protection device was found to have improved 1-month outcomes in one randomized controlled trial of distal protection devices, but neither the device alone nor antiplatelet therapy alone had this benefit.87 Further study is warranted to determine the role of distal protection therapies and devices.
Pathology of Renal Infarction
Renal infarction is a relatively infrequent clinical diagnosis, but common finding at autopsy. In a review of over 14,000 autopsies from Los Angeles County Hospital in the 1930s, renal infarctions were noted in 1.4%, and were most often postmortem diagnoses.88 Renal infarctions most commonly occur with arterial occlusions, but may occur in venous thrombosis. The size of the infarct depends on the size of the occluded artery and may be a small wedge-shaped infarct or may involve the entire kidney. The gross appearance of the infarct depends on the size of the occluded artery, age of the infarct, and presence or absence of infection. In the first few hours the infarct is red and pyramidal, and subsequently becomes gray with a narrow red rim of congested parenchyma. The area shrinks, leaving behind a V-shaped scar. Infarctions typically involve only the renal cortex, sparing the medulla.89
TABLE 56.2 Clinical and Laboratory Features of Thromboembolic Diseases of the Kidney
On microscopic examination, sterile infarcts have the classical picture of coagulative necrosis.89 The initial findings of marked congestion are followed by cytoplasmic and nuclear degenerative changes, with gradual loss of viable cytologic structure. The cytoplasm becomes homogeneous and eosinophilic, and the nuclei undergo condensation and karyorrhexis. Surrounding this necrotic area is a transitional zone of sublethal injury with findings similar to acute tubular necrosis. This peripheral area becomes infiltrated with polymorphonuclear leukocytes. Eventually the central necrotic area becomes smaller, with eventual collapse, and is replaced by a collagenous scar.89
Clinical Features and Diagnosis of Acute Occlusive Renal Arterial Disease
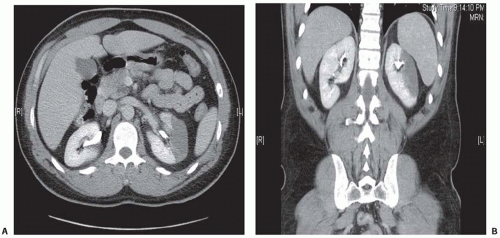
There are no definitive signs or symptoms specific for arterial occlusion (Table 56.2). The most common presenting symptom for arterial occlusion of the kidney is pain, which may be flank and/or abdominal pain. Other nonspecific symptoms may include nausea, vomiting, or fever and chills. Anuria or oliguria is usually suggestive of bilateral arterial occlusion, or unilateral occlusion in patients with a solitary kidney, but transient oliguria lasting a few days may occur in unilateral occlusion as well. This oliguria has been attributed to arteriolar spasm of the contralateral kidney. The size of the infarct may impact the severity of pain as in one small series of iatrogenic renal infarcts following endovascular procedures, the patients were all asymptomatic, with the infarctions being discovered by routine CT imaging.84 Because of the relative infrequency with which it occurs compared to more common intra-abdominal pathology such as gastroenteritis, pancreatitis, pyelonephritis, and nephrolithiasis, renal infarction may not be among diagnostic considerations in the initial workup, and diagnosis may be delayed. Unfortunately this may lead to irreversible loss of renal function. With increasing reliance on abdominal imaging by CT scan as part of initial diagnostic evaluations for patients presenting to emergency departments with abdominal pain, this pattern may change in the future with more events being discovered earlier in the evaluation. Figure 56.1 demonstrates transverse and coronal CT images of a renal infarction.
Other physical findings may be elevated blood pressure. Bowel sounds may be diminished. Abdominal and/or flank tenderness are often present on physical examination. With smaller infarcts, there may be no signs or symptoms.
FIGURE 56.1 Computed tomography with contrast. Transverse (A) and coronal (B) images demonstrate a wedge-shaped embolic infarct localized to the lateral midpole of the left kidney.
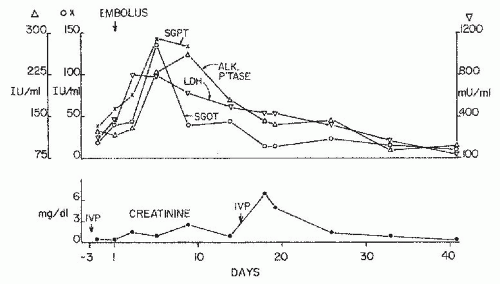
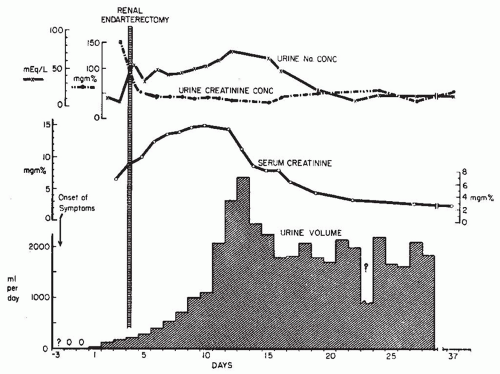
The most common laboratory abnormality is elevation in LDH, with levels that reach as high as 2,000 IU per L. Other associated laboratory abnormalities include elevation in serum AST, ALT, and alkaline phosphatase, but these are typically less dramatic and are not universally noted. Microscopic hematuria, leukocytosis, and mild proteinuria are common findings.90 Reduced urinary excretion of sodium, as is commonly noted in renal hypoperfusion, is also noted at times.91 The course of changes in LDH, AST, ALT, and alkaline phosphatase in a patient are noted in Figure 56.2, with changes in urine volume, serum creatinine, and urine sodium noted in Figure 56.3.92
FIGURE 56.2 Serial serum levels of glutamic-oxaloacetic transaminase (SGOT, ○)glutamic-pyruvic transaminase (SGPT, X), lactic dehydrogenase (LDH, δ), alkaline phosphatase (ALK P TASE, δ), and creatinine (•) in a 62-year-old man with thromboembolism to a single kidney 10 days after a myocardial infarction. Right flank and chest pain and lower abdominal tenderness appeared on day 1. The patient also exhibited an increase in serum creatinine level following the second intravenous pyelogram (IVP). (From Lessman RK, Johnson SF, Coburn JW, et al. Renal artery embolism: clinical features and long-term follow-up in 17 cases. Ann Intern Med. 1978;89:477, with permission.)
FIGURE 56.3 Course of a 56-year-old woman with abrupt onset of anuria and right lower quadrant and low back pain; she had atrial fibrillation and mitral stenosis owing to rheumatic heart disease. One year earlier she had undergone a left nephrectomy for malignant hypertension. (Earlier, she had had a stroke and blindness of the left eye owing to an embolism.) A diagnosis of thromboembolism to the renal artery was confirmed by aortography (Fig. 56.4), and surgery was performed with removal of the embolus and endarterectomy. The fractional excretion of sodium was 0.36% before surgery and increased to 7.3% after removal of the thrombus. There was ultimate recovery from acute tubular necrosis, as indicated. (From Lessman RK, Johnson SF, Coburn JW, et al. Renal artery embolism: clinical features and long-term follow-up in 17 cases. Ann Intern Med. 1978;89:477, with permission.)
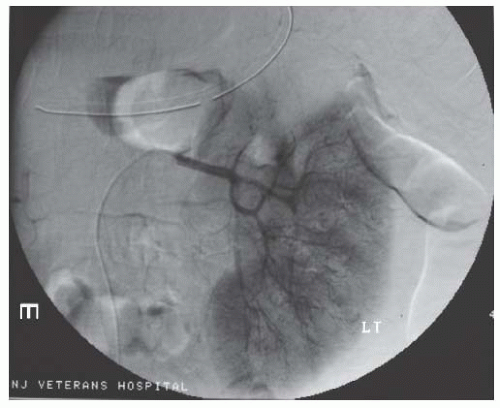
CT scan with contrast is probably the most rapid, widely available, and reliable imaging modality. Magnetic resonance angiography may also be useful, but may take longer and is not as widely available. Angiography is of course the most accurate diagnostic method, and holds the additional advantage of allowing rapid endovascular intervention or thrombolytic therapy for an acute occlusion, and should be considered as a first line test if clinical suspicion is high. A characteristic angiographic image of renal infarct is shown in Figure 56.4. Nuclear medicine renal flow scans can also be used to identify isolated perfusion defects (Figure 56.5), but if isotope uptake is globally reduced (as can be seen in acute kidney injury) it may fail to identify an area of hypoperfusion. Ultrasonography of the renal arteries is of limited value as it is time consuming, operator-dependent, and difficult to image the entire renal artery, although for cases of transplant renal artery thrombosis or for thrombosis of the main renal artery, it may have some utility.93
Therapy for Nontraumatic Acute Occlusive Renal Arterial Disease
Similar to traumatic renal arterial occlusion, the major concern is irreversible loss of renal function, and likewise the response to therapy depends on the duration of warm ischemia, location, and severity of the occlusion and presence or absence of collateral circulation. Acute thromboembolic events may be amenable to intraarterial thrombolytic therapy, and a timely diagnosis is crucial to preserve renal function.
Blum et al. published a series of 14 patients with acute embolic renal artery occlusion treated with thrombolytic therapy.94 The estimated ischemic time varied from 12 hours to 8 days. Although renal perfusion was restored in 13 of the patients, this did not translate into recovery of renal function. None of the patients with complete occlusion had restoration of renal function, but the patients with partial occlusion were stabilized. Their review of 50 cases of complete renal artery occlusion suggested a warm ischemia duration of 3 hours or less in order to preserve renal function without permanent injury.94 This “critical ischemia time” has been refuted by a number of isolated case reports who achieved good clinical outcomes even after delayed restoration of renal perfusion.95,96,97,98,99 Several of the cases described duration of ischemia longer than 20 hours and in one case of an elderly patient with solitary functioning kidney, satisfactory renal recovery occurred despite a 4-day history of occlusion with anuria and a temporary dialysis requirement.97
FIGURE 56.4 Left renal angiogram shows a wedge-shaped perfusion defect involving the upper pole of the kidney due to a thromboembolism.
Surgical treatment of acute occlusive renal arterial disease has produced mixed results. Lacombe described a series of 20 patients (5 with acute embolism, and 15 with acute thrombosis) who underwent surgical revascularization between 18 hours and 68 days after the occlusion. Kidney salvage rate was 64%, but postoperative mortality was 15%. A number of these patients may have had underlying renal artery stenosis with development of collateral circulation that may have led to a better rate of renal preservation.100 Another series reported by Ouriel et al. describes 13 patients in whom renal artery embolectomy failed to restore renal function.101
Much as is the case for traumatic thrombosis, the decision to intervene on patients with acute nontraumatic thrombosis or thromboembolism should be based on duration and extent of ischemia and identification of patients most likely to benefit. Patients with substantial risk of significant loss of renal function, such as those with bilateral occlusion, or unilateral occlusion of a solitary kidney, should be considered for revascularization. Patients with a normal contralateral kidney or smaller infarctions may be better served by more conservative therapy. Another clinical decision is the need for short- or long-term systemic anticoagulation. There are no guidelines specifically oriented toward anticoagulation for renal arterial thrombosis or thromboembolic disease. A decision for systemic anticoagulation should be based on subsequent risk of further embolic events, such as with atrial fibrillation or severe ventricular dysfunction.
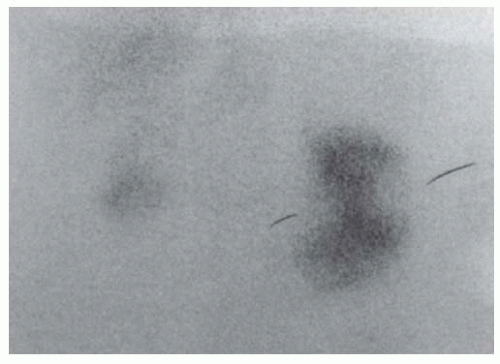
FIGURE 56.5 Renal scan with technetium 99m-labeled dimercaptosuccinic acid (DMSA) showing evidence of segmental renal infarcts of the left kidney of a 74-year-old man who was hospitalized with abrupt appearance of a supraventricular tachycardia. There was a progressive rise in serum creatinine from a baseline value of 2.2 to 4.4 mg/dL over 5 successive days. He was never oliguric; urinalysis showed 2+ proteinuria. His white blood cell count rose from 10,200/µL on admission to 15,400/µL after 4 days; there was no eosinophilia. The serum alanine aminotransferase level rose from 33 to 42 U/L and lactate dehydrogenase, from 49 to 173 U/L. A technetium-labeled “flow” scan disclosed markedly reduced flow bilaterally that was more marked on the left than the right. There was a history of emboli to his feet, with the serum creatinine level increasing from 1.2 to 2.2 mg/dL in association with an acute myocardial infarction several years ear-lier. On the basis of DMSA scan, a diagnosis of thromboembolism to the kidney was made; the patient received anticoagulants and his serum creatinine level gradually fell to 2.4 mg/dL.
RENAL ARTERY ANEURYSMS
Renal artery aneurysms (RAAs) are uncommon in the general population. Autopsy studies report a prevalence in the general population of around 0.01%.102,103 In patients undergoing renal arterial angiography (to evaluate hypertension for example) the prevalence is between 0.3% and 1.3%.104,105,106,107 One series of 8525 renal angiograms identified RAAs in 83 patients (0.97%).102 Of these, 80% were saccular, 61% were right-sided, and 7% were bilateral.
Renal artery aneurysms can be classified as saccular, fusiform, dissecting, and intrarenal.106,108 Saccular aneurysms are the most common and account for 80% of renal artery aneurysms. They are typically located at the first-order bifurcation of the main renal artery. Less than 10% are within the renal parenchyma.
Fusiform aneurysms are less common, and most commonly noted in an area following stenosis, giving the appearance of poststenotic dilatation.32,109,110,111,112 Fusiform aneurysms are responsible for the “string of beads” appearance of some cases of fibromuscular dysplasia, where several stenotic areas are followed by dilatations.
Intrarenal aneurysms make up 10% to 15% of RAAs. They may be congenital, posttraumatic (e.g., following renal biopsy), or associated with polyarteritis nodosa.110,113
Histologic findings of RAAs resemble medial fibromuscular dysplasia. In the arterial wall, degeneration of the internal elastic lamina with fragmentation, increased collagen, and a lack of elastic tissue are observed. Atherosclerotic lesions may be the cause of the aneurysm or, more likely, may be a secondary factor.114 Calcification of the arterial walls may occur.
Table 56.3 shows demographic and clinical data of 277 patients undergoing surgical correction of renal aneurysms from three published series.114,115,116 The mean age was 50 years (range 13 to 78). Women outnumbered men by 65% to 35% and hypertension was common, in >70% of the patients. Medial fibromuscular dysplasia was considered the major cause (34% to 54%) and was the presumed reason for the female gender preference. Atherosclerosis was noted in 25% to 35%. Small numbers of patients had renal artery aneurysms due to polyarteritis nodosum, giant cell arteritis, Marfan syndrome, dissection, mycotic aneurysms, and trauma.114,115,116,117,118
TABLE 56.3 Data from Three Large Studies Reporting Their Surgical Outcomes of Renal Artery Aneurysms in 277 Patients
a English WP, Pearce JD, Craven TE, et al. Surgical management of renal artery aneurysms. J Vasc Surg. 2004;40:53-60.
b Pfeiffer T, Reiher L, Grabitz K, et al. Reconstruction for renal artery aneurysm: operative techniques and long-term results. J Vasc Surg. 2003;37:293-300.
c Henke PK, Cardneau JD, Welling TH, 3rd, et al. Renal artery aneurysms: a 35-year clinical experience with 252 aneurysms in 168 patients. Ann Surg. 2001;234:454-462; discussion 62-63.
RAA, renal artery aneurysm.
The most serious complication of renal artery aneurysms is rupture, which can quickly lead to hemorrhagic shock, loss of renal function, and death.119 Other complications may include dissection (discussed later in this section) and thrombosis with distal embolization. Embolization can further result in formation of an arteriovenous fistula with resultant high-output heart failure.108,109 Most patients with RAAs are asymptomatic, although some may complain of nonspecific flank or abdominal pain, and there may be hematuria or abdominal bruit on assessment.
Rupture of renal artery aneurysms is a potentially catastrophic event and may quickly lead to hemorrhagic shock, irreversible loss of kidney function, and death. It is typically accompanied by severe flank pain and flank ecchymoses. For unclear reasons rupture of RAAs occurs disproportionately in pregnancy. Because of the relative infrequency of renal artery aneurysm, there are no prospective data regarding risk of rupture, but individuals at higher risk are felt to be those with larger aneurysms (particularly those >4.0 cm) and with aneurysms during pregnancy. There have been some prospective data regarding natural history of smaller aneurysms. Two-hundred patients, mostly with RAAs less than 2.0 cm, were managed conservatively for up to 17 years.102,104,114,120,121,122 None of them ruptured during follow-up and very few caused symptoms or increased substantially in size. Henriksson et al. reported a series of 34 patients with RAAS undergoing periodic angiographic surveillance.120 Twenty-eight of the patients experienced no change in the size, five had slight enlargement, and one patient underwent surgical repair to address a worrisome dilation. These observational data suggest that, for smaller aneurysms, conservative management with interval imaging studies is a reasonable management approach.
Pregnant women with RAAs represent a unique group in which conservative therapy may not be appropriate. In a review of 43 cases of RAA rupture, 18 (42%) occurred in pregnant women.122 Most ruptures occur during the third trimester, but there have been case reports of rupture earlier in pregnancy and also in the postpartum period.119,123,124,125
There has also been a report during pregnancy of a ruptured renal artery aneurysm involving a transplanted kidney.126 The explanation for increased risk of rupture during pregnancy is not clear. Most of the pregnant women who experienced rupture did not have hypertension before or during the pregnancy.123,127,128 Some of the proposed contributing factors include increased renal blood flow, particularly during the third trimester, steroid hormone effects, and increased intra-abdominal pressure.127 Pressure on the pelvic vasculature, which may be positional, is also felt to be a potential contributor.123,128,129 Cases of RAA rupture during pregnancy typically require emergent nephrectomy to control hemorrhage. Maternal mortality is 6% and fetal mortality 25% if the pregnancy has reached the third trimester.130 Fetal mortality approaches 100% in cases before the third trimester.
The most sensitive imaging study for renal artery aneurysm is angiogram. Magnetic resonance angiography (MRA) may be a useful technique depending on the size and location of the aneurysm. CT may be useful as a screening tool as well. For detection of smaller, more distal or intrarenal aneurysms, angiogram may be the only useful imaging modality.
Patients undergoing surgical repair of RAAs in one of three large published series have demonstrated good surgical outcomes. In a combined number of 277 patients undergoing repair of aneurysms with a mean size of 1.6 to 2.6 cm, primary surgical success was 97% and long-term arterial patency ranged from 81% to 91%.114,115,116 One of the centers reported a rate of unplanned nephrectomy of 6.6% (8 of 121 surgeries). Two of the series reported data about hypertension outcomes and reported improvement in hypertension in 20% to 50% and “cure” in 20% to 25%.115,116 Perioperative death rate was 0% to 1.6% and morbidity 12% to 17%. Because of the complexity of the surgery, referral to an experienced surgical team is recommended for successful outcome.
Only gold members can continue reading. Log In or Register to continue
May 29, 2016 | Posted by drzezo in NEPHROLOGY | Comments Off on Renal Artery Thrombosis, Thromboembolism, Aneurysms, Atheroemboli, and Renal Vein Thrombosis