undergoing CCPD use an automated cycler to perform exchanges while they sleep with a subsequent “last fill” and single daytime dwell until the following evening; therefore, this is a continuous therapy. Some patients also require a daytime exchange, either to maximize solute clearances or to enhance fluid removal. Although it may be done manually, this exchange is more commonly performed using the cycler as a “docking” station for drain of the last fill instilled in the morning and subsequent instillation of fresh dialysis fluid. APD performed in this fashion is commonly referred to as CCPD with a midday exchange or as “high-dose” CCPD (a misnomer, as the volume of fluid used may well be less than that used by another patient performing “low” dose CCPD).
TABLE 83.1 Goals of End-Stage Renal Disease Replacement Therapy | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
TABLE 83.2 Solute Removal by Dialysis and the Natural Kidney | |||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||
clearance, within the range achieved in clinical practice, do not result in significant improvement in patient morbidity or mortality (Table 83.3).52,53 This accumulating body of data should not be taken to mean that peritoneal clearances are biologically irrelevant or that providing peritoneal clearances do not have a survival benefit—an anuric patient would die in the absence of peritoneal clearances. However, these data clearly suggest that within the range of clearances currently achieved in clinical practice, higher peritoneal clearances are unlikely to result in significant improvement in patient survival.
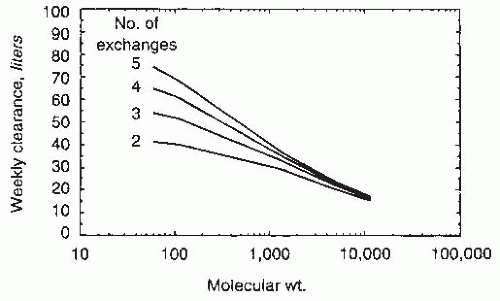 FIGURE 83.1 The influence of the number of exchanges on the weekly solute clearance for solutes with a range of molecular weights derived from a computerized model of peritoneal transport. (From Keshaviah P. Adequacy of CAPD: a quantitative approach. Kidney Int Suppl. 1992;38:S160, with permission.) |
On the other hand, it appears from outcome studies that the Kt/Vurea target may not need to change. Furthermore, it is now recognized that the stronger relationship of creatinine clearances to patient outcome was a result of the effect of the confounding effect of residual renal function. There is no evidence that peritoneal creatinine clearances are superior in predicting outcome, when compared to peritoneal urea clearance. In light of these considerations, the various expert groups recommend the use of Kt/Vurea alone to determine the dose of dialysis (Table 83.4). Second, the targets for Kt/Vurea have been changed, such that Kt/Vurea of 1.7 at all times is now considered to be the minimum dose necessary needed for patient well-being. Based on the results of the two recent randomized controlled trials, it is also recognized that some patients may require a higher dose of dialysis to manage uremic symptoms or to achieve euvolemia.36,37 Third, except in the CARI guidelines, there are no differences in the definition of minimum dose of dialysis based upon the patients’ transport type (see below). Fourth, some expert groups (Europe and Australia) have defined the adequacy of dialysis based only on peritoneal clearances, whereas others (Canada and the United States) define it based upon total clearances. Fifth, the targets are the same, irrespective of PD modality (CAPD or APD). Finally, volume control is recognized as an additional dimension to define adequate dialysis (see below).
TABLE 83.3 Summary of Randomized, Controlled Clinical Trials That Have Evaluated the Effect of Increasing Dialytic Clearances on Outcome among Patients Undergoing Peritoneal Dialysis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 83.4 Targets for Small Solute Clearances Recommended by Various Organizations for Patients Undergoing Chronic Peritoneal Dialysis | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||
are measured. For each dwell time (0, 120, and 240 minutes), dialysate to plasma ratios (D/P) of creatinine and urea are determined, as is the ratio of glucose at the drain time (120 and 240 minutes) to the initial dialysate glucose concentration (D/ D0). These results are plotted against time and compared to known standard curves (Fig. 83.2). Based on the values of D/P creatinine or D/D0 glucose, patients are classified into one of four categories: low, low average, high average, and high transporters. It should be noted that there is a significant discordance between the categorization of patients’ transport type, based upon whether D/P creatinine or D/D0 glucose is used (Fig. 83.3).72 Studies suggest that abbreviating the preceding exchange to 2 to 3 hours does not significantly influence the values of D/P creatinine or D/D0 glucose; thus, patients being treated with APD do not have to change their treatment schedule on the day prior to the PET.73,74
TABLE 83.5 Tests to Evaluate Peritoneal Membrane Function | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
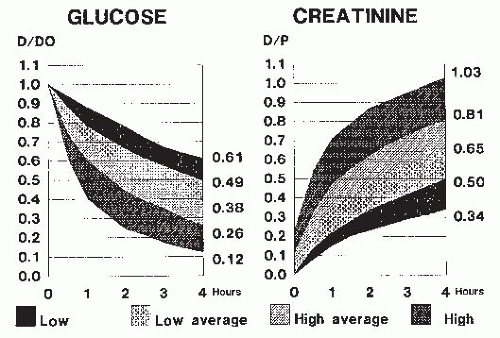 FIGURE 83.2 Dialysate to plasma ratios (D/P) for creatinine and drain time to initial dialysis concentration (D/D0) ratios for glucose, generated from standard peritoneal equilibration testing. (From Twardowski ZJ. Clinical value of standardized equilibrium tests in CAPD patients. Blood Purif. 1989;7:95, with permission.) |
D/P creatinine and high D/D0 glucose). The D/P ratios for creatinine and urea increase almost linearly during the dwell. For these patients, dwell time is the crucial determinant of overall clearance. They do best with continuous therapies, such as standard CAPD or CCPD. Notwithstanding these considerations, the vast majority of patients have an “average” transport type and they can be successfully treated with either PD modality. Two recent, large studies have demonstrated that there is not a difference in mortality among patients treated with CAPD or APD.78,79 Furthermore, either PD modality (CAPD or CCPD) can be successfully adapted to even patients at the extreme of transport type (rapid or slow).
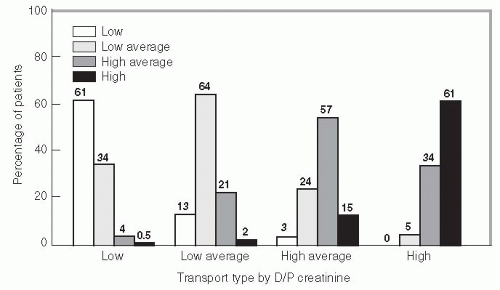 FIGURE 83.3 Discordance between categorization of patients’ transport type by D/P creatinine or D/D0 glucose. Thus, of the patients categorized low transporter by D/P creatinine, 61% of them will be classified as a low transporter by D/D0 glucose; of the patients classified as low average transporter, 64% will be classified as low average transporter by D/D0 glucose; of the patients classified as high average transporter, 57% will be classified as high average transporter by D/D0 glucose; and of the patients classified as high transporter by D/P creatinine, 61% will be classified as high transporter by D/D0 glucose. (Modified from Mujais S, Vonesh E. Profiling of peritoneal ultrafiltration. Kidney Int Suppl. 2002;81:S17, with permission.) |
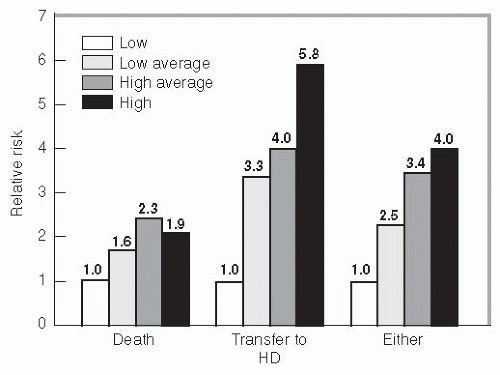 FIGURE 83.4 Relationship between transport type and patient outcome. With increasing permeability of the peritoneum, as defined by the peritoneal equilibration test, there is an increasing risk for death and/or technique failure. (Modified from Churchill DN, Thorpe KE, Nolph KD, et al. Increased peritoneal transport is associated with poor patient and technique survival on continuous ambulatory peritoneal dialysis. J Am Soc Nephrol. 1998;9:1285.) |
TABLE 83.6 Commonly Used Formulas for Protein Nitrogen Appearance | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
TABLE 83.7 Strategies to Enhance the Peritoneal Small Solute Clearances | ||||||
|---|---|---|---|---|---|---|
|









