Upper Tract Obstruction, Loin Pain, Hydronephrosis
Hydronephrosis
Dilatation of the renal pelvis and calyces (Fig. 10.1). When combined with dilatation of the ureters, known as hydroureteronephrosis.
Obstructive nephropathy is damage to the renal parenchyma, resulting from an obstruction to the flow of urine anywhere along the urinary tract.
Dilatation of the renal pelvis and calyces can occur without obstruction and therefore, hydronephrosis should not be taken to necessarily imply the presence of obstructive uropathy.
Ultrasound
False negative (i.e. obstruction present, no hydronephrosis): acute onset of obstruction; in the presence of an intrarenal collecting system; with dehydration; misdiagnosis of dilatation of the calyces as renal cortical cysts (in acute ureteric colic, ultrasonography fails to detect hydronephrosis in up to 35% of patients with proven acute obstruction on IVU).
Diagnostic approach to the patient with hydronephrosis
Patients with hydronephrosis may present either as an incidental finding of hydronephrosis on USS or CT done because of non-specific symptoms or it may be identified in a patient with a raised creatinine or presenting with loin pain. Symptoms, if present, will depend on the rapidity of onset of obstruction of the kidney (if that is the cause of the hydronephrosis), whether the obstruction is complete or partial, unilateral or bilateral, and whether the obstruction to the ureter is extrinsic to the ureter or is within its lumen.
History
Severe flank pain suggests a more acute onset of obstruction and if very sudden in onset, a ureteric stone may well be the cause. Pain induced by a diuresis (e.g. following consumption of alcohol) suggests a possible PUJO.
Anuria (the symptom of bilateral ureteric obstruction or complete obstruction of a solitary kidney).
If renal function is impaired, symptoms of renal failure may be present (e.g. nausea, lethargy, anorexia).
Extrinsic causes of obstruction (e.g. compression of the ureters by retroperitoneal malignancy) usually have a more insidious onset whereas intrinsic obstruction (ureteric stone) is often present with severe pain of very sudden onset.
An increase in urine output may be reported by the patient due to poor renal concentrating ability.
Obstruction in the presence of bacterial UTI—signs and symptoms of pyelonephritis (flank pain and tenderness, fever) or sepsis.
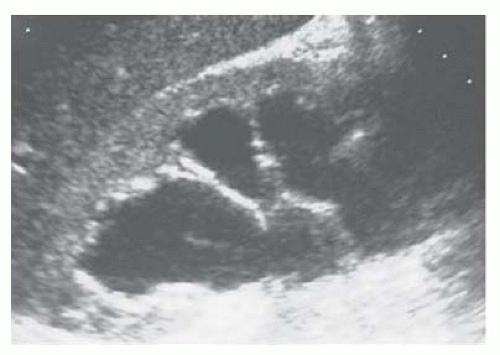 Fig. 10.1 Hydronephrosis as seen on renal ultrasonography. |
Examination
Bilateral oedema (due to fluid overload).
Abdominal examination: percuss and palpate for an enlarged bladder.
DRE (? prostate or rectal cancer) and, in women, vaginal examination (? cervical cancer).
Check serum creatinine to determine the functional effect of the hydronephrosis.
Renal ultrasonography (if not already done).
IVU findings in renal obstruction
An obstructive (dense) nephrogram.
A delay in filling of the collecting system with contrast material.
Dilatation of the collecting system.
An increase in renal size.
Rupture of fornices (junction between renal papilla and its calyx) with urinary extravasation.
Ureteric dilatation and tortuosity.
A standing column of contrast material in the ureter.
Unilateral hydronephrosis
If no stone seen, but hydronephrosis is confirmed and ureter is non-dilated, the obstruction must be at the PUJ. In the absence of a ureteric stone visible on CTU, the diagnosis must be PUJO.
If no stone seen and the ureter is dilated as well as the kidney, ureteric TCC is likely. Arrange retrograde ureterography to identify site of obstruction and ureteroscopy/ureteric biopsy.
Bilateral hydronephrosis
If the patient is in retention or has a substantial post-void residual urine volume, pass a catheter. If the elevated creatinine falls (and the hydronephrosis improves), the diagnosis is BOO due, for example, to BPH, prostate cancer, urethral stricture, DSD. If the creatinine remains elevated, the obstruction affecting both ureters is higher ‘upstream’.
Causes of hydronephrosis
Unilateral
Bilateral
BOO.
Bilateral ureteric obstruction at their level of entry into the bladder.
Locally advanced cervical cancer.
Locally advanced prostate cancer.
Locally advanced rectal cancer.
Poor bladder compliance (often combined with DSD): neuropathic bladder (spinal cord injury, spina bifida), post-pelvic radiotherapy.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree




