Following fertilization, a blastocyte (sphere of cells) is created, which implants into the uterine endometrium on day 6. The early embryonic disc of tissue develops a yolk sac and amniotic cavity, from which are derived the ectoderm, endoderm, and mesoderm. Organ formation occurs between 3 and 10 weeks’ gestation. Most of the genitourinary tract is derived from the mesoderm.
Upper urinary tract
The pronephros (precursor of the kidney; pro = (Gk) before) is derived from an intermediate plate of mesoderm, which functions between weeks 1-4. It then regresses. The mesonephros (meso = (Gk) middle) functions from weeks 4-8 and is also associated with two duct systems—the mesonephric duct and adjacent to this, the paramesonephric duct (para = (Gk) beside) (Fig. 16.1a). The mesonephric (Wolffian) ducts develop laterally and advance downwards to fuse with the cloaca (Latin = sewer), a part of the primitive hindgut. By week 5, ureteric buds grow from the distal part of the mesonephric ducts and by a process of reciprocal induction, they stimulate the formation of the metanephros (permanent kidney; meta = (Gk) after) when they reach the renal tissue. Branching of the ureteric bud forms the ureter, renal pelvis, calyces, and collecting ducts. Glomeruli and nephrons (distal convoluted tubules, proximal convoluted tubules, and loop of Henle) are derived from metanephric mesenchyme (metanephros). During weeks 6-10, the caudal end of the fetus grows rapidly and the fetal kidney effectively moves up the posterior abdominal wall to the lumbar region. Urine production starts at week 10.
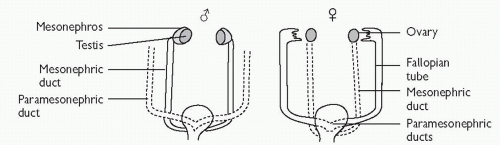
Thus, in both males and females, the mesonephric duct forms the ureters and renal collecting system. The paramesonephric duct essentially forms the female genital system (Fallopian tubes, uterus, upper vagina); in males, it regresses. The mesonephric ducts also form the male genital duct system (epididymis, vas deferens, seminal vesicles) and central zone of the prostate; in females, it regresses (see p. 648).
Lower urinary tract
Bladder
The mesonephric ducts and ureters drain into the cloaca. During weeks 4-6, the cloaca is subdivided into the urogenital canal or sinus (anteriorly) and the anorectal canal (posteriorly) by a process of growth, differentiation, and remodelling (Fig. 16.1b).1 The bladder is formed by the upper part of the urogenital canal. Bladder smooth muscle (detrusor) is developed from adjacent pelvic mesenchyme. The trigone develops separately, arising from a segment of the mesonephric duct. The bladder dome is initially connected to the allantois, but this connection later regresses to become a fibrous cord (urachus).
Urethra
The inferior portion of the urogenital canal forms the entire urethra in females and the posterior urethra in males. Closure of the urogenital groove creates the male anterior urethra. The mesonephric ducts separate from the ureters (Fig. 16.1c) and travel caudally to join the posterior urethra in males (where they differentiate into the male genital duct system at 8-12 weeks).
Fig. 16.1 (a) Development of the upper urinary tract; (b) Development of the lower urinary tract (bladder); (c) Development of the distal ureters and mesonephric ducts.
1 Penington EC, Hutson JM (2003) The absence of lateral fusion in cloacal partition. J Paediatr Surg38:1287-95.
Embryology: genital tract
Sexual differentiation and gonadal development is determined by the sex chromosomes (XY, male; XX, female). The gonads produce hormones which influence the subsequent differentiation of internal and external genitalia.
Both sexes
Gonads develop from the genital ridges (formed by cells of the mesonephros and coelomic epithelium). At 5-6 weeks, primordial germ cells migrate from the yolk sac to populate the genital ridges. Primitive sex cords are formed, which support germ cell (sperm and ova) development.
From 4 weeks, the mesonephric (Wolffian)ducts are incorporated into the genital system when renal function is taken over by the definitive kidney. At 6 weeks, coelomic epithelium creates the paramesonephric (Müllerian) ducts which develop laterally and are fused to the urogenital sinus at their bases.
Males
Embryos are genetically programmed to be female unless the testisdetermining gene (SRY) is present, in which case the embryo will differentiate into a male. The SRY gene is located on the Y chromosome. It stimulates medullary sex cords in the primitive testis to differentiate into Sertoli cells which produce Müllerian inhibiting substance (MIS) at 7-8 weeks. The sex cords differentiate into seminiferous cords, which later form the seminiferous tubules of the testis within which the primordial germ cells differentiate into spermatogonia. MIS triggers regression of the paramesonephric ducts, testosterone secretion from Leydig cells of the testis, and the initial phase of testicular (abdominal) descent. The androgens testosterone and dihydrotestosterone (DHT) are responsible for masculinization of the fetus.
During weeks 8-12, the mesonephric ducts differentiate into the epididymis, vas deferens, seminal vesicles, and ejaculatory ducts. Under the influence of DHT, proliferation and budding of the urethral endoderm gives rise to prostatic acini and glands and by a process of reciprocal induction, forms the prostatic capsule and smooth muscle from the surrounding mesenchyme (completed by week 15).
After week 23, the second androgen-dependent phase of testicular descent occurs. The testes rapidly descend from the abdomen (via the inguinal canal during weeks 24-28) and into the scrotal sac, aided by calcitonin gene-related polypeptide acting on the gubernaculum. The testis is enclosed in a diverticulum of peritoneum called the processus vaginalis. The distal part persists as the tunica vaginalis around the testis, the remainder usually regresses.
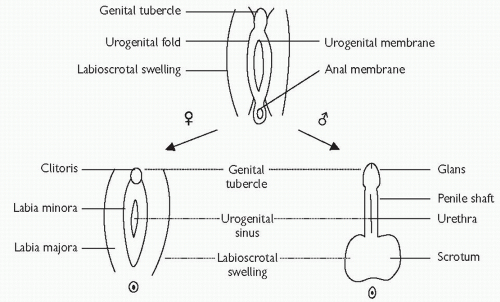
External genitalia develop from week 7. Urogenital folds form around the opening of the urogenital sinus and labioscrotal swellings develop on either side. The penile shaft and glans are formed by elongation of the genital tubercle and fusion of urogenital folds. The scrotum is created by fusion of labioscrotal folds.
The genital ridge forms secondary sex cords (primitive sex cords degenerate) which surround the germ cells to create ovarian follicles (week 15). These undergo meiotic division to become primary oocytes which are later activated to complete gametogenesis at puberty. Oestrogen is produced from week 8 under the influence of the aromatase enzyme. In the absence of MIS, the mesonephric ducts regress and the paramesonephric ducts become the Fallopian tubes, uterus, and upper two-thirds of the vagina. The sinovaginal sinus is developed at the junction of the paramesonephric ducts and the urogenital sinus. This forms the lower third of the vagina.
The genital tubercle forms the clitoris; the urogenital folds become the labia minora and the labioscrotal swellings form the labia majora.
Fig. 16.2 Differentiation of external genitalia (weeks 7-16).
Fig. 16.3 Differentiation of the genital tract.
Undescended testes (UDT)
The first phase of testicular descent from the genital ridge to internal inguinal ring occurs under the influence of MIS acting on the gubernaculum (around 7-8 weeks’ gestation). The second phase of testicular descent through the inguinal canal into the scrotum occurs at 24-28 weeks’ gestation under the influence of testosterone. Failure of descent results in cryptorchidism or congenital UDT.
Incidence
Four percent at birth for a full-term neonate, however, many will spontaneously descend after birth and the incidence at 1y is 1.3-1.8%. The incidence of unilateral UDT is greater than bilateral UDT.
Classification
Retractile: an intermittent active cremasteric reflex causes the testis to retract up and out of the scrotum.
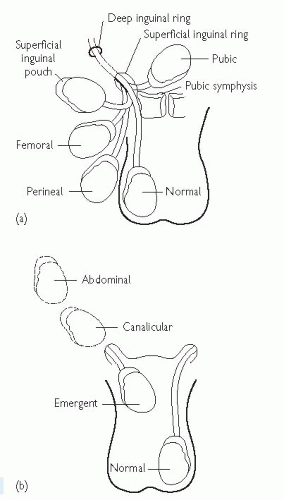
Ectopic (<5%): abnormal testis migration below the external ring of the inguinal canal (to perineum, base of penis, or femoral areas) (Fig. 16.4).
Incomplete descent (˜95%): testis may be intra-abdominal, intra-inguinal, or pre-scrotal (Fig. 16.4).
Atrophic/absent.
Acquired UDT (or testicular ascent): testes that were down in the scrotum have ascended. Risk higher with retractile testes and a patent processus vaginalis. It occurs around 7-9y old and the incidence is 1-2%.1 Approximately 20% will fail to return to the scrotum by puberty. Orchidopexy is recommended as the ‘ascended’ testis is at the same risk of degenerative changes as congenital UDT.
Risk factors
Preterm infants (incidence at <30 weeks’ gestation is 40%).
UDT demonstrate the degeneration of Sertoli cells, loss of Leydig cells, atrophy, and abnormal spermatogenesis. Male fertility depends on the transformation of gonocytes to dark adult spermatocytes within the first 3 months of post-natal life. This appears to be defective in UDT.
Long-term complications
Relative risk of cancer is 8-fold higher in UDT. There is a 4% lifelong risk of cancer with an intra-abdominal testis. Majority are seminomas. There is a slightly increased risk of cancer in the contralateral, normally descended testis.
Reduced fertility (paternity rate in unilateral UDT is 80-90% and in bilateral UDT is 45-65%). Paternity rates improve if orchidopexy is performed before 2y of age.
Increased risk of testicular torsion or trauma.
Increased risk of indirect inguinal hernias (due to a patent processus vaginalis).
Evaluation
Examine the scrotum and inguinal region to elucidate if a testis is palpable and to identify its location. Retractile testes may be brought back down into the bottom of the scrotum without tension. Assess for associated congenital defects. If neither testis is palpable, consider chromosome analysis (to exclude an androgenized female) and endocrine analysis (high LH and FSH with a low testosterone indicates anorchia, confirmed with serum inhibin B). For the impalpable testis, USS is of limited use. Most proceed directly to examination under anaesthetic ± diagnostic laparoscopy and treatment.
Treatment
Inguinal UDT: is treated with orchidopexy between 6-18 months old. Surgery consists of inguinal exploration, mobilization of spermatic cord, ligation of processus vaginalis, and securing the testis into a dartos pouch in the scrotal wall. Risks include testicular atrophy (5%), damage to vas (1-2%), and re-ascent of the testis.
Intra-abdominal testes: require a laparoscopic approach to mobilize the testis for orchidopexy as a single or 2-stage (Fowler-Stephens) procedure. The Fowler-Stephens approach involves initial clipping or division of spermatic vessels to provide extra length (the testis then relies on collateral blood flow from the vas). Six months later, the testis is then mobilized on its vas with its new collateral vessels and brought down into the scrotum. Success rates are ˜85%. Intra-abdominal testes with a short vas may need microvascular autotransplantation. This involves high intra-abdominal ligation of the spermatic vessels, the testis is brought down into the scrotum, and the vessels are re-anastomosed to the inferior epigastric vessels. Small, atrophic intra-abdominal testes (nubbin) require orchidectomy ± orchidopexy of the contralateral normally descended testis.
Overall success rates of orchidopexy vary according to position of the UDT: 92% for inguinal testes, 87% for canalicular testes, and 74% for abdominal testes.3
Fig. 16.4 (a) Ectopic sites for the undescended testis; (b) Incomplete descent of the testis (Reproduced with permission from Taylor & Francis Books, UK).
1 Hack WW, Sijstermans K, van Dijk J, et al. (2007) Prevalence of acquired undescended testis in 6-year, 9-year and 13-year-old Dutch schoolboys. Arch Dis Child;92:17-20.
2 Brewster S, Cranston D, Noble J, Reynard J (2001) Urology a Handbook for Students. BIOS Scientific Publishers Limited.
3 Docimo SG (1995) The results of surgery for cryptorchidism: a literature review and analysis. J Urol154:1148-52.
Urinary tract infection (UTI)
Definitions:UTI is a bacterial infection of the urine, which may involve the lower urinary tract/bladder (cystitis) or upper urinary tract/kidney (pyelonephritis) (see p. 176).
Classification: children may be asymptomatic or symptomatic. Simple UTI: presents with mild dehydration and pyrexia.
Severe UTI: presents as fever ≥38°C, unwell, vomiting, with moderate to severe dehydration.
Atypical UTI: includes features of serious illness/septicaemia, poor urinary flow, abnormal renal function, failure to respond to treatment in <48h, and non-E. coli infection.
Recurrent UTI: in children, describes either one episode of cystitis with one episode of pyelonephritis, ≥2 episodes of pyelonephritis, or ≥3 episodes of cystitis. It may be due to bacterial persistence, unresolved infection, or re-infection.
Incidence: up to age 1, the incidence in boys is higher than girls (male: female ratio is 3:1), but thereafter, the incidence in girls becomes greater (school age males 1%; females 3%).
Pathology: common bacterial pathogens are E. coli, Enterococcus, Pseudomonas, Klebsiella, Proteus, and S. epidermidis. Bacteria enter via the urethra to cause cystitis and ascending infection causes pyelonephritis. Alternatively, there can be haematogenous spread from other systemic infections.
Risk factors
Age: neonates and infants have increased bacterial colonization of the periurethral area and an immature immune system.
Foreskin: uncircumcised boys have a 10-fold higher risk of UTI in the first year due to bacterial colonization of the glans and foreskin.
Faecal colonization: contributes to perineal bacterial colonization.
Chronic constipation.
Presentation
Neonates and infants: fever, irritability, vomiting, lethargy, diarrhoea, poor feeding, failure to thrive, abdominal pain, offensive urine, haematuria.
Children: fever, nausea, suprapubic pain, dysuria, frequency, voiding difficulties, changes to continence, abdominal or flank pain, haematuria.
Investigation
Urine analysis and culture: advised with unexplained fever ≥38°C or if symptomatic of UTI. Clean catch specimen where possible. In toilettrained children, an MSU specimen is considered diagnostic with ≥105 colony-forming units (CFU)/mL in asymptomatic children and ≥104CFU/mL if symptomatic. In young children, a catheterized urine specimen with ≥10CFU/mL) of one pathogen or a suprapubic aspirate with ≥102CFU/mL are diagnostic of UTI. Collection bag specimens are less reliable due to skin flora contamination.
USS is the first-line investigation. It identifies bladder and kidney abnormalities (hydronephrosis, stones).
DMSA renogram can demonstrate and monitor renal scarring.
MCUG detects urethral and bladder anomalies (anatomical and functional), VUR, and ureteroceles.
Management
Infants <3 months (and children at risk of serious illness): are managed according to the ‘feverish illness in children’ guidelines.2 For children aged 3 months to 3y, antibiotics are recommended (before urine culture results are available) for specific symptoms of UTI and for non-specific symptoms where the risk of intermediate to serious infection is high (i.e. associated anatomical or functional abnormality).2 In children older than 3y, antibiotics are indicated if urine dipstick analysis is positive for nitrites ± leukocyte esterase or if there is good clinical evidence of UTI.
Infants <3 months: paediatric referral and treat with IV antibiotic such as third-generation cephalosporin (cefotaxime or ceftriaxone).2
Infants and children >3 months with pyelonephritis: paediatric referral; 7-10 days of oral cephalosporin or co-amoxiclav or IV cefotaxime or cefriaxone for 2-4 days followed by oral antibiotics for a total of 10 days.
Infants and children >3 months with cystitis: oral antibiotics for 3 days (trimethoprim, nitrofurantoin, cephalosporin, or amoxicillin), and reassess. The choice of antibiotics should be directed by local hospital guidelines.
Asymptomatic bacteriuria does not require antibiotics or routine follow-up. Antibiotic prophylaxis is not recommended following a firsttime simple UTI, but can be considered after recurrent symptomatic UTI.3 Advice on preventing UTI should be given, including good intake of fluids, regular voiding, and treatment of constipation.
Follow-up: recurrent UTI or abnormal imaging requires paediatric assessment. Long-term follow-up is needed for bilateral renal anomalies, impaired renal function, hypertension, and/or proteinuria. Follow-up should include recordings of growth (height, weight), BP, and urine dipstick testing.
Table 16.1 Recommended imaging regimen for infants <6 months1
1 National Institute for Health and Excellence (2007) Urinary tract infection: diagnosis, treatment and long-term management of urinary tract infection in children [online]. Available from: http://www.nice.org.uk/CG54.
2 National Institute for Health and Excellence (2007) Feverish illness in children—assessment and initial management in children younger than 5 years [online]. Available from: http://www. nice.org.uk/CG047.
3 Williams G, Craig JC (2011) Long-term antibiotics for preventing recurrent urinary tract infection in children. Cochrane Database Syst Rev3:CD001534.
Antenatal hydronephrosis
Definition
Generally defined as a maximal anteroposterior renal pelvis diameter (RPD) of ≥5mm on antenatal USS.
Incidence
The incidence of antenatal hydronephrosis (RPD ≥5mm) is approximately 0.6% on second trimester (20 weeks’ gestation) USS. The incidence of antenatal USS-detected congenital anomalies of the urinary tract is 0.1-4%. An increasing degree of hydronephrosis is related to increased risk of urinary tract pathology and requirement for surgery.1, 2 However, in around 65%, antenatal hydronephrosis will resolve and overall, <5% will require nephrological or surgical intervention.3
Aetiology
Causes include transient hydronephrosis (48%), physiological hydronephrosis (15%), PUJO, VUR, megaureter, multicystic dysplastic kidney (MCDK), renal cysts, posterior urethral valves (PUV), ectopic ureter, and ureterocele (also see Table 16.4).3
Table 16.4 Clinically significant causes of antenatal hydronephrosis3
Bilateral hydroureteronephrosis and distended, thick-walled bladder, dilated posterior urethra, oligohydramnios, and pulmonary hypoplasia
Antenatal management
20 weeks’ gestation USS. If necessary, repeat the scan to observe for changes when the bladder empties. Note the gender of fetus.
Repeat USS later in pregnancy if hydronephrosis to assess for persisting or increasing renal dilatation.
Antenatal counselling to discuss differential diagnosis, prognosis, and investigations required post-natally. Particularly important for BOO (i.e.PUV), unilateral RPD >30mm, bilateral RPD >15mm, MCKD, and ureterocele.
Arrange delivery at an appropriate centre for cases requiring specialist intervention (i.e. with paediatric urology, nephrology, and neonatal ITU on site).
General principles of post-natal management
Specific post-natal investigation and management will depend on the underlying diagnosis and severity of hydronephrosis and are described individually later in this chapter. The important principles of post-natal management include:
Clinical assessment, including BP reading. Examine for a palpable bladder (PUV), abdominal mass (PUJO, MCKD).
Start prophylactic antibiotics immediately (trimethoprim 2mg/kg daily) until the diagnosis is established. Exceptions to this include: RPD <10mm and normal calyces (give UTI advice); MCDK with normal contralateral kidney and ectopic kidney with no dilatation.
Renal function blood tests (particularly if distended bladder, ureterocele, bilateral hydronephrosis, and unilateral hydronephrosis in a solitary kidney).
Imaging
Post-natal USS: generally recommended at 1 and 6 weeks’ postnatal,3 although it can be delayed longer for lower risk anomalies. If possible, avoid USS in the first 48h post-delivery as normal urine output is only established after this time. Exceptions that require immediate USS are conditions with obstruction needing urgent surgery—PUV and ureterocele.
MCUG: is deferred until the child is older (˜3-6 months) unless there is an urgent clinical indication (BOO/PUV) where it is performed as soon as possible after birth. Other indications for MCUG include duplex kidney, ureterocele, and renal scarring,4 where it is used to detect associated VUR.
DMSA: is a static scan which provides an accurate measurement of renal split function. It is used to confirm non-function of multicystic kidney, differential function of upper and lower moieties of a duplex kidney, and renal damage associated with VUR and UTI (renal cortical scarring). It is performed at 6-12 weeks old.
MAG3: is a dynamic scan used to identify obstruction where there is no demonstrable reflux and significant hydronephrosis persists (RPD >10mm). Usually deferred until the infant is 6-12 weeks old. It also provides an approximation of renal split function and is particularly useful for the diagnosis of PUJO.
Consider urgent referral to paediatric urology for:
(Please refer to local hospital guidelines as these will differ between different hospitals and tertiary centres.)
1 Passerotti CC, Kalsih LA, Chow J, et al. (2011) The predictive value of the first postnatal ultrasound in children with antenatal hydronephrosis. J Pediatr Urol7:128-36.
2 Grignon A, Filiom R, Filiatrault D, et al. (1986) Urinary tract dilatation in utero. Classification and clinical application. Radiology160:645-7.
3 Woodward M, Frank D (2002) Postnatal management of antenatal hydronephrosis. BJU Int89:149-56.
4 Mears AL, Raza SA, Sinha AK, Misra D (2007) Micturating cystourethrograms are not necessary for all cases of antenatally diagnosed hydronephrosis. J Pediatr Urol3:264-7.
Vesicoureteric reflux (VUR)
Definition:VUR results from abnormal retrograde flow of urine from the bladder into the upper urinary tract.
Pathogenesis: the ureter passes obliquely through the bladder wall (1-2cm) where it is supported by muscular attachments which prevent urine reflux during bladder filling and voiding. The normal ratio of intramural ureteric length to ureteric diameter is 5:1. Reflux occurs when the intramural length of ureter is too short (ratio <5:1) (Paquin’s law). The degree of reflux is graded I-V (see p. 408; Fig. 8.3). The appearance of the ureteric orifice changes with increasing severity of reflux, classically described as stadium, horseshoe, golf hole, or patulous.
Only gold members can continue reading. Log In or Register to continue
 p. 648).
p. 648).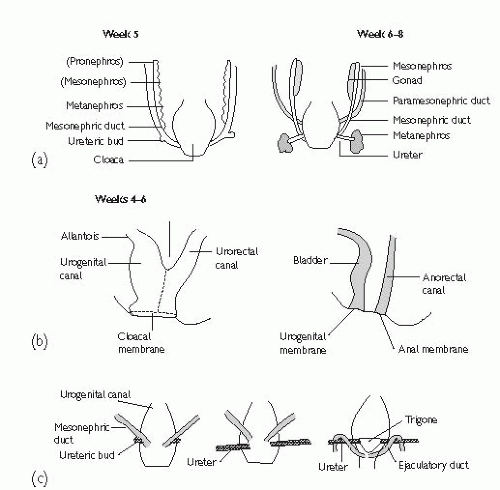
 p. 176).
p. 176).
 http://www.nice.org.uk/CG54.
http://www.nice.org.uk/CG54. http://www. nice.org.uk/CG047.
http://www. nice.org.uk/CG047.





 p. 408; Fig. 8.3). The appearance of the ureteric orifice changes with increasing severity of reflux, classically described as stadium, horseshoe, golf hole, or patulous.
p. 408; Fig. 8.3). The appearance of the ureteric orifice changes with increasing severity of reflux, classically described as stadium, horseshoe, golf hole, or patulous.





