grade 2 tumors (WHO 1973) into the high-grade papillary carcinoma category.13,17,18 For example, in the study by Yin and Leong,18 13 of 46 WHO (1973) grade 2 tumors (28%) were placed in the WHO (2004) high-grade category resulting in 23% of all cases being considered high-grade in WHO 2004 compared to only 4% being called grade 3 in the 1973 WHO system. Similarly, Samaratunga et al.17 reviewed 134 papillary tumors of which 6 (4%) had been reported as grade 3 (WHO, 1973); on review they considered 29 (22%) to be high grade by WHO/ISUP 1998.
Table 6-1 ▪ 1973 WHO GRADING CRITERIA | ||||||||
|---|---|---|---|---|---|---|---|---|
| ||||||||
Table 6-2 ▪ 2004 WHO/1998 ISUP CLASSIFICATION | |||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||
invasive disease has been reported to be <1%.31, 32, 33 In these studies, the one case with progression was on immunosuppressive therapy following renal transplantation.
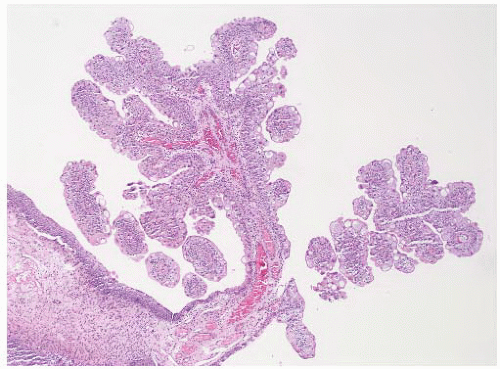 FIGURE 6-1 ▪ Urothelial papilloma showing a small tumor with fine papillary fronds. |
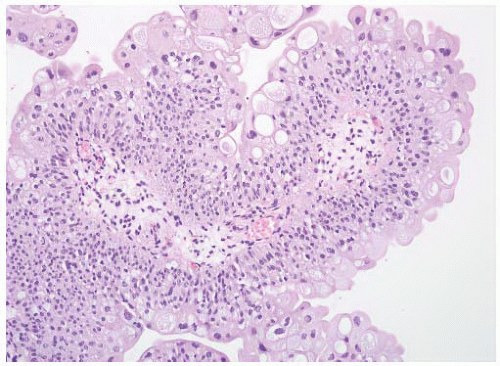 FIGURE 6-2 ▪ Urothelial papilloma with the surface urothelium showing no cytologic or architectural atypia. |
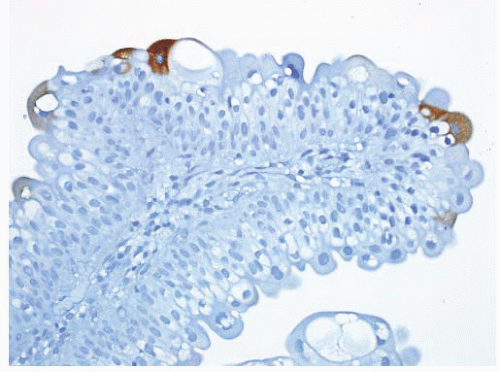 FIGURE 6-3 ▪ Urothelial papilloma with immunohistochemistry for cytokeratin 20 highlighting a few umbrella cells. |
entity that occurs over a wide age range but most often after the age of 50.5,40, 41, 42, 43, 44, 45, 46, 47 They are much more common in men than women. These develop throughout the urinary tract but are most common in the urinary bladder, in particular the trigone and bladder neck region. Cases of synchronous inverted papilloma and papillary carcinoma are well described though rare. In rare cases, they can be multifocal.42 Inverted papilloma is treated by transurethral resection and is associated with a low risk of recurrence (<5%) that is distinctly different from low-grade papillary urothelial neoplasms.42,43
|
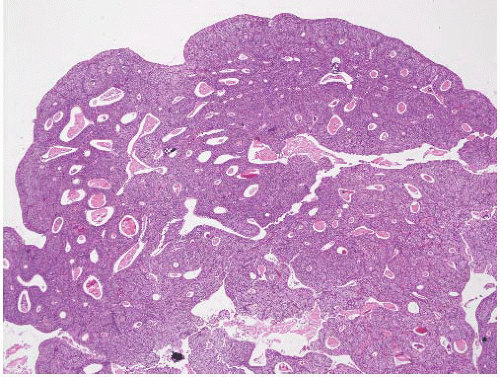 FIGURE 6-4 ▪ Inverted urothelial papilloma with polypoid appearance, flattened surface epithelium, and complex trabecular architecture. |
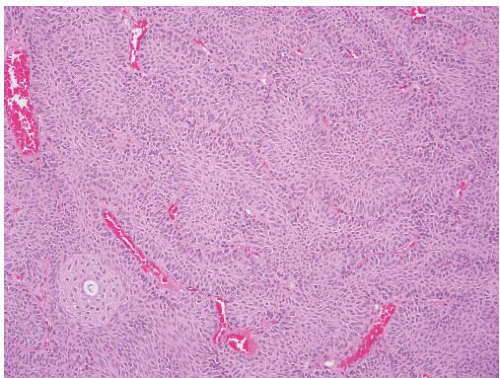 FIGURE 6-5 ▪ Inverted urothelial papilloma with palisading of basilar cells and streaming of centrally located cells. |
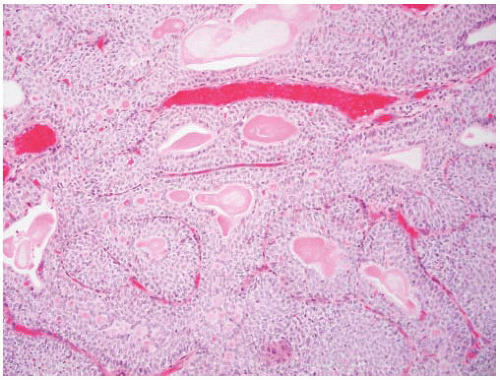 FIGURE 6-6 ▪ Inverted urothelial papilloma with glandular spaces lined by columnar epithelium. |
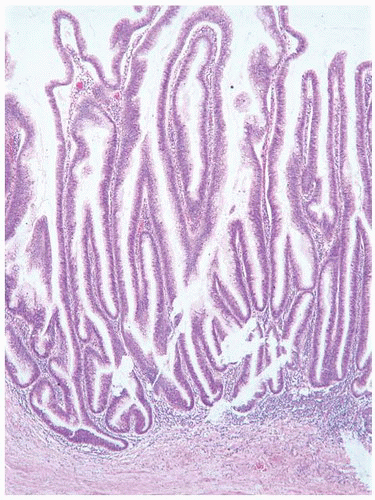 FIGURE 6-7 ▪ Villous adenoma with tall villiform papillae. |
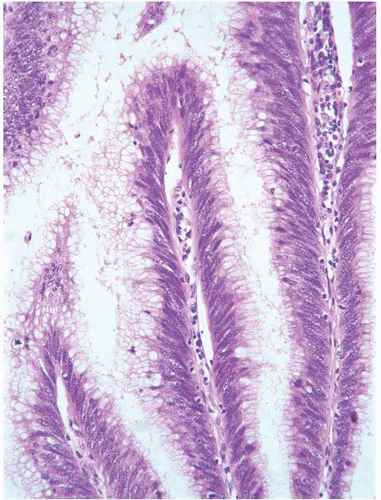 FIGURE 6-8 ▪ Villous adenoma with pseudostratified mucinsecreting epithelium. |
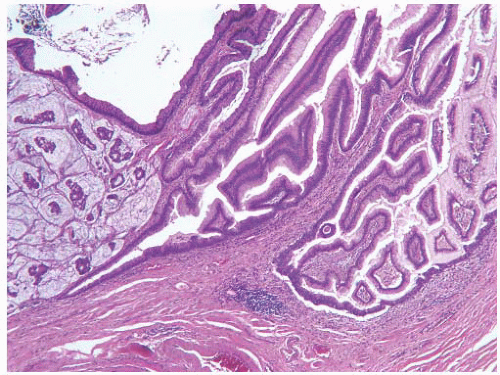 FIGURE 6-9 ▪ Villous adenoma with associated mucinous adenocarcinoma. |
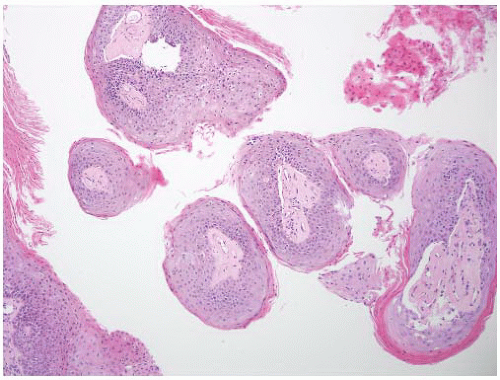 FIGURE 6-10 ▪ Squamous papilloma with fine papillary structures covered by keratinizing squamous epithelium. |
Table 6-3 ▪ UROTHELIAL CARCINOMA: IMPLICATED CARCINOGENIC AGENTS | ||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||
TP53, retinoblastoma (RB), and PTEN.102 Both the RB and TP53 genes have generated intense interest in bladder cancer. RB gene deletions are common in high-grade bladder tumors and have been associated with an aggressive clinical course.115 The absence of RB protein or inactivation of RB protein affects multiple critical pathways including the E2F family of transcription factors. As in the case of RB, the importance of the TP53 tumor suppressor gene has been extensively studied in bladder cancer. TP53 mutations are present in up to 70% of urothelial carcinomas and are related to high-grade and high-stage disease and also to poor clinical outcome.116 Studies related to loss of chromosome 9 in CIS have had variable results103; in one report chromosome 9 loss was significantly higher in primary CIS than in CIS associated with papillary tumors.117 The TP53 mutation analysis demonstrated a similar relationship suggesting that these might represent two different types of CIS.103 FGFR3 mutations are not present in primary CIS and are infrequent in CIS associated with papillary tumors.106,118
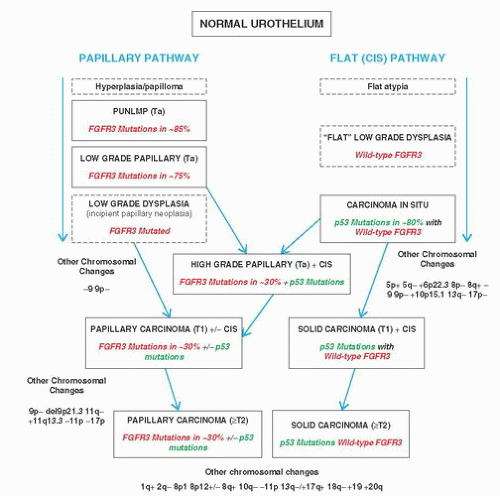 FIGURE 6-11 ▪ Pathways for the development of urothelial tumors. |
obstruction, a pelvic mass, or obstruction of pelvic lymphatics. Least common are presentation as a metastasis of unknown origin or general cancer cachexia.
Table 6-4 ▪ URINE-BASED MARKERS FOR BLADDER CANCER | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
of the tumor. The general approach to resection of a tumor (TURBT, transurethral resection of bladder tumor) is to first remove the bulk or entirety of the tumor and second to sample the base of the tumor. These may be submitted as a single specimen or as two separately designated specimens. In situations where the complete resection of the lesion is not possible or not indicated, the urologist should be removing sufficient tissue for accurate diagnosis and staging (meaning evaluation of the muscularis propria). The procedure is usually performed with an instrument that cauterizes the remaining surface as the tissue fragments are removed. Depending on instrument settings, this can result in a considerable degree of artifact that can hamper interpretation of tissue specimens removed. The degree of tissue artifact is not related to the use of unipolar or bipolar energy.167
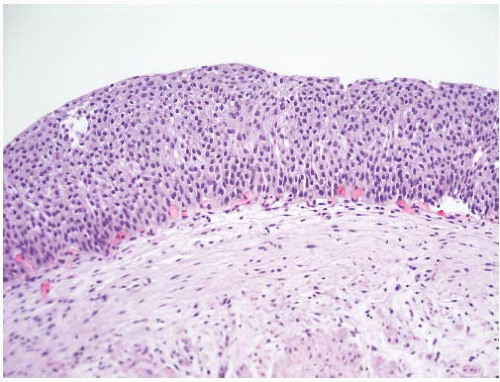 FIGURE 6-12 ▪ Urothelial hyperplasia with thickened epithelium lacking any architectural or cytologic atypia. |
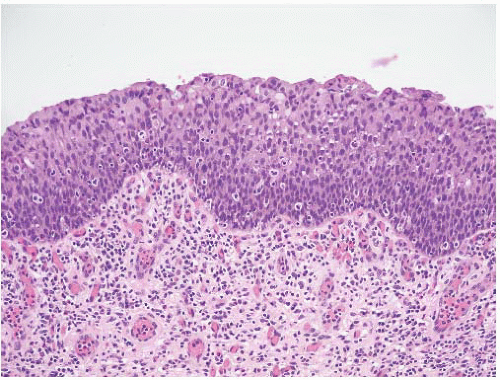 FIGURE 6-13 ▪ Reactive urothelial atypia with thickened epithelium, no architectural atypia, and mildly enlarged nuclei, many containing small nucleoli. |
Table 6-5 ▪ MORPHOLOGIC FEATURES OF FLAT LESIONS | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
lesions into only two categories: urothelial dysplasia and urothelial CIS. Urothelial dysplasia has been divided into primary dysplasia for when the lesion is diagnosed de novo and secondary dysplasia when it is found in the setting of known urothelial neoplasia.174 There is evidence, largely genetic, that it shares some abnormalities with CIS and therefore likely represents a precursor lesion.175
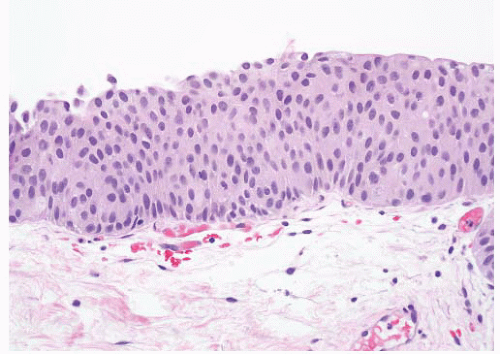 FIGURE 6-14 ▪ Urothelial dysplasia with flat epithelium showing a mild degree of architectural and cytologic atypia. |
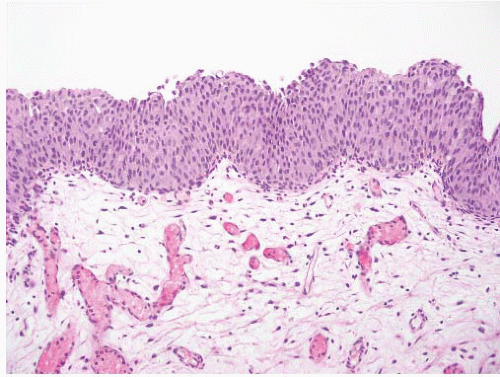 FIGURE 6-15 ▪ Urothelial dysplasia with slight tenting of the surface. |
CIS of the bladder in patients with other urothelial tumors is also important.192 The risk of having CIS in the upper tract is three- to four-fold higher and in the prostatic urethra is seven-fold higher than when a bladder tumor does not have associated CIS.193,194 For patients with noninvasive papillary tumors, the presence of CIS is associated with a higher risk of recurrence and progression.195 In cases with lamina propria invasion (T1), the presence of CIS also indicates an increased risk of progression to muscle-invasive disease and has been used as one of the indications for early cystectomy.195,196
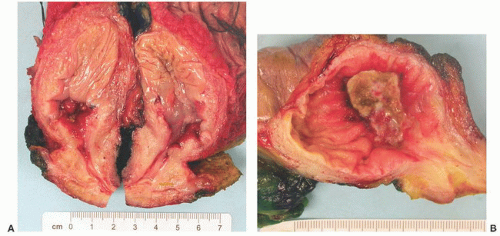 FIGURE 6-16 ▪ Gross appearance of CIS localized to area around an invasive carcinoma (A) and more diffusely involving the mucosa (B). |
Table 6-6 ▪ MORPHOLOGIC PATTERNS OF UROTHELIAL CIS | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
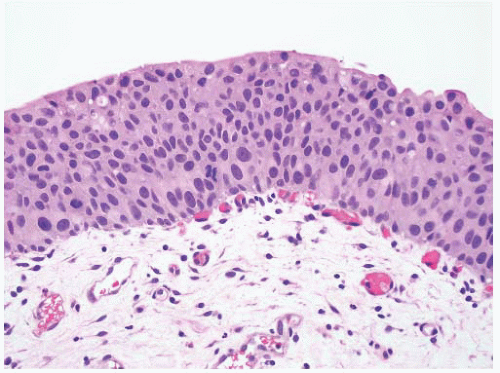 FIGURE 6-17 ▪ Urothelial CIS with haphazardly arranged cells with significant nuclear pleomorphism. |
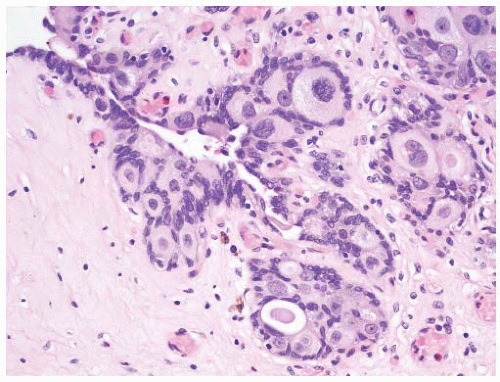 FIGURE 6-18 ▪ Urothelial CIS showing pagetoid spread into von Brunn nests. |
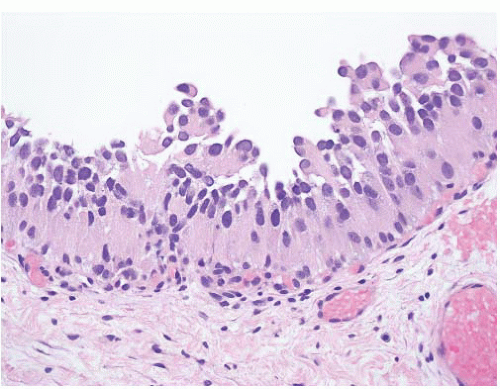 FIGURE 6-19 ▪ Urothelial CIS with cells having abundant eosinophilic cytoplasm. |
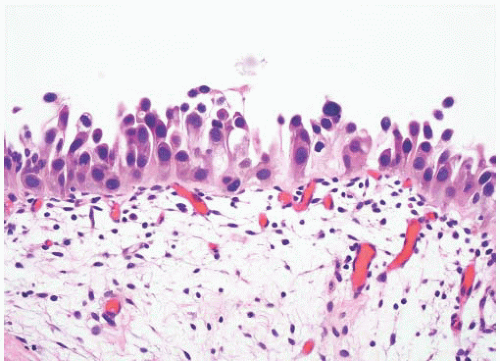 FIGURE 6-20 ▪ Urothelial CIS with a denuding pattern. |
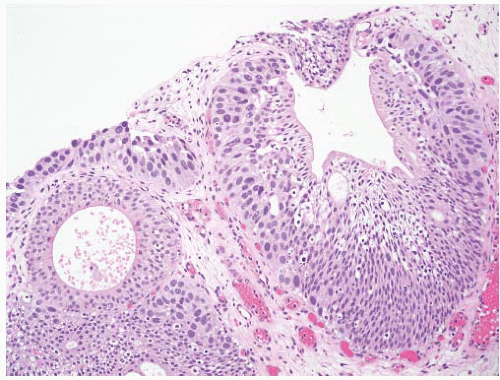 FIGURE 6-21 ▪ Urothelial CIS spreading into von Brunn nest and lifting the overlying benign urothelium. |
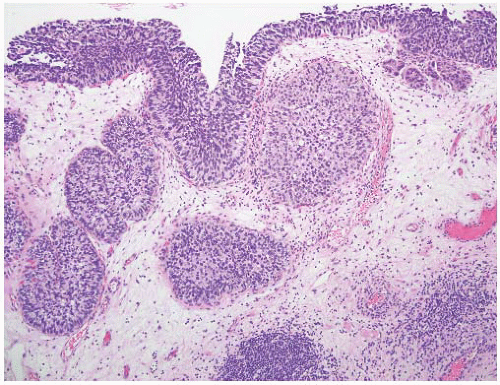 FIGURE 6-22 ▪ Urothelial CIS extending into and expanding von Brunn’s nests simulating an invasive tumor. There is a small focus of early invasion in the upper right. |
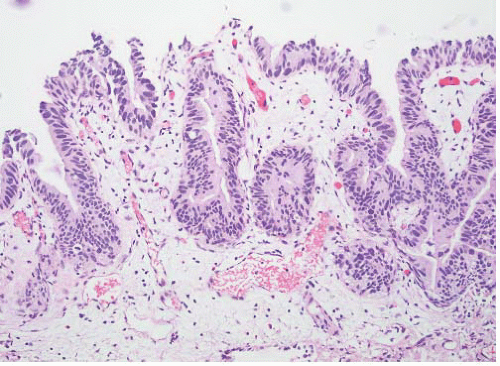 FIGURE 6-23 ▪ Urothelial CIS with cells having fusiform nuclei mimicking adenocarcinoma in situ. |
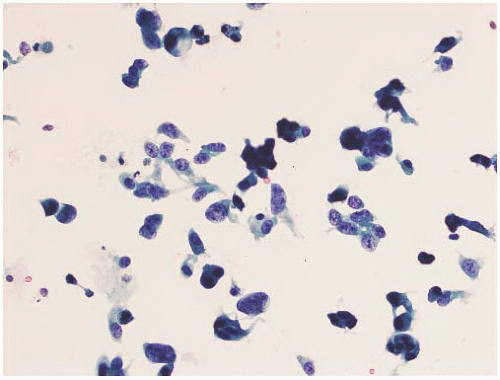 FIGURE 6-24 ▪ Urothelial CIS in a bladder wash specimen with discohesive individual malignant cells. |
30% in normal epithelium. The high frequency of abnormalities in histologically benign urothelium limits the application of this approach.
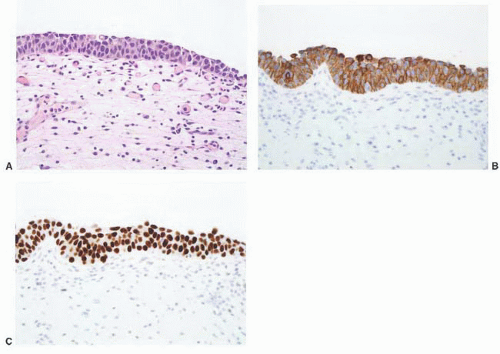 FIGURE 6-25 ▪ Urothelial CIS with malignant cells forming a thin epithelium (A). Immunohistochemistry shows diffuse reactivity for cytokeratin 20 (B) and p53 (C). |
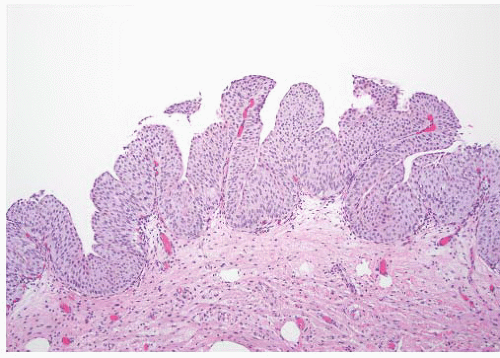 FIGURE 6-26 ▪ Papillary urothelial carcinoma with short papillary fronds. |
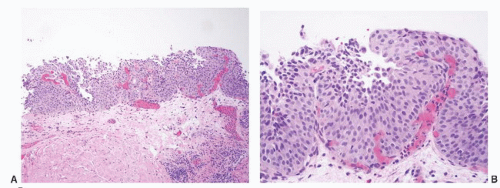 FIGURE 6-27 ▪ Papillary urothelial carcinoma with early formation of identifiable papillae (A,B). |
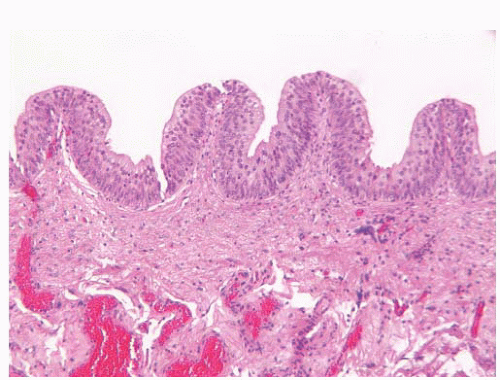 FIGURE 6-28 ▪ Prominent tenting of the mucosal surface producing pseudopapillae (papillary hyperplasia). |
 FIGURE 6-29 ▪ Small, single papillary urothelial carcinoma on the posterior wall of the bladder. |
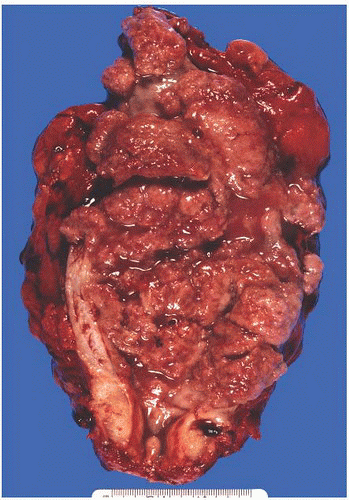 FIGURE 6-30 ▪ Diffuse involvement of the bladder by noninvasive (pTa) low-grade papillary urothelial carcinoma. |
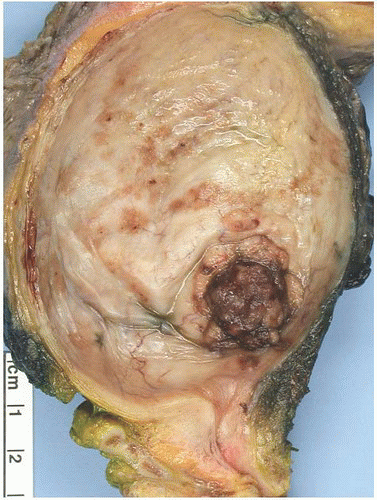 FIGURE 6-31 ▪ Invasive (pT2a), high-grade papillary urothelial carcinoma. |
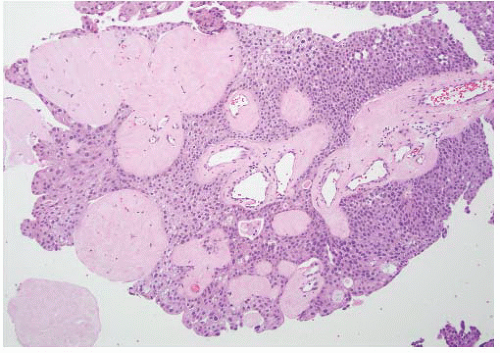 FIGURE 6-32 ▪ Papillary urothelial carcinoma with hyalinization of the papillary cores. |
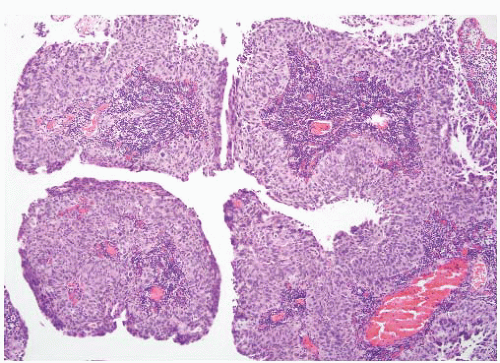 FIGURE 6-33 ▪ Papillary urothelial carcinoma with intense chronic inflammatory infiltrate in the papillary cores. |
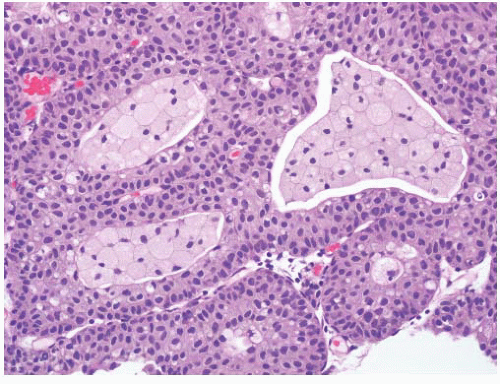 FIGURE 6-34 ▪ Papillary urothelial carcinoma with foamy macrophages in the papillary cores. |
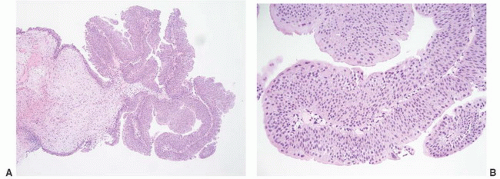 FIGURE 6-35 ▪ Papillary urothelial neoplasm of low malignant potential at low (A) and high (B) magnification. |
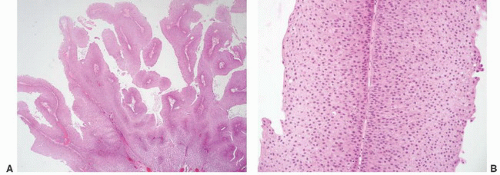 FIGURE 6-36 ▪ Papillary urothelial neoplasm of low malignant potential at low (A) and high (B) magnification. |
These tumors have a significantly higher recurrence rate than for papillary urothelial neoplasm of low malignant potential and similar to high-grade papillary carcinomas.9 They also have a higher rate of stage progression than papillary urothelial neoplasm of low malignant potential but significantly lower than for high-grade papillary carcinoma.9,19,34 Low-grade tumors can be invasive though this is distinctly uncommon. A review of the literature revealed a mean recurrence rate of 50% and mean stage progression rate of 10%.13 In the large series of Pan et al.213 these accounted for 60% of noninvasive papillary tumors and had recurrence and progression rates of 35% and 6.5%, respectively. At last follow-up, 2% of patients presenting with low-grade papillary carcinoma had died of bladder cancer.213 Patients with these tumors require close clinical follow-up though recently it has been suggested that this can be less frequent than for patients with high-grade tumors.21 A single dose of intravesical therapy (most often mitomycin-C) is optional but maintenance intravesical therapy is not recommended.23
Table 6-7 ▪ PAPILLARY UROTHELIAL NEOPLASMS: ARCHITECTURAL FEATURES | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||
Table 6-8 ▪ PAPILLARY UROTHELIAL NEOPLASMS: NUCLEAR FEATURES | ||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||
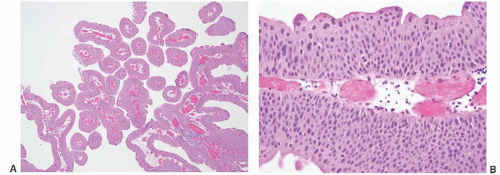 FIGURE 6-37 ▪ Low-grade papillary urothelial carcinoma at low (A) and high (B) magnification. |
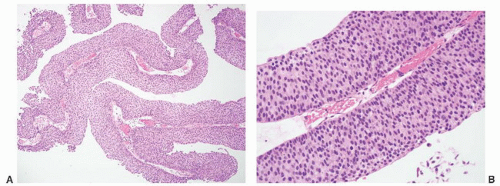 FIGURE 6-38 ▪ Low-grade papillary urothelial carcinoma at medium (A) and high (B) magnification. |
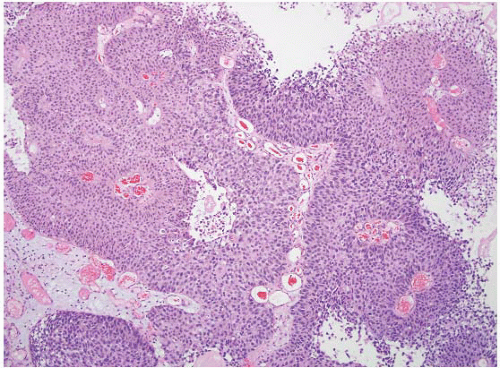 FIGURE 6-39 ▪ Papillary urothelial carcinoma with low-grade (left) and high-grade (right) areas. |
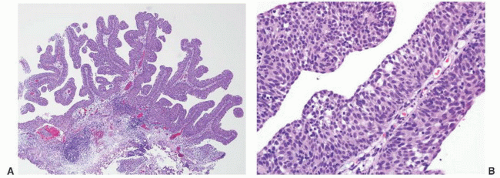 FIGURE 6-40 ▪ High-grade papillary urothelial carcinoma at low (A) and high (B) magnification. |
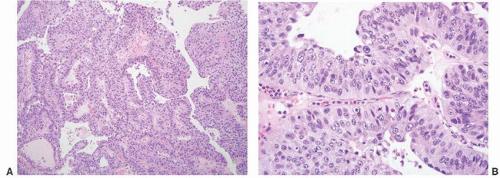 FIGURE 6-41 ▪ High-grade papillary urothelial carcinoma at low (A) and high (B) magnification. |
is homogeneous and lacks vacuolization. Mitoses are absent or infrequent.
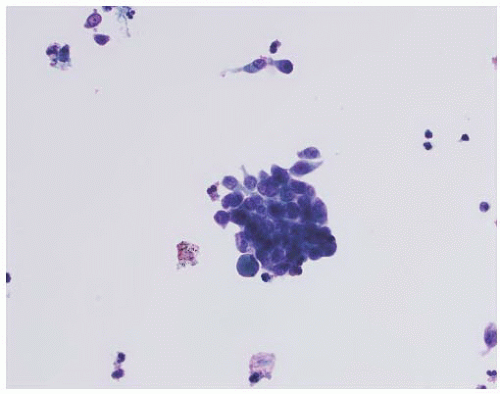 FIGURE 6-42 ▪ Bladder washing specimen from a low-grade papillary urothelial carcinoma. |
Table 6-9 ▪ MIMICS OF PAPILLARY NEOPLASMS | ||||||
|---|---|---|---|---|---|---|
|
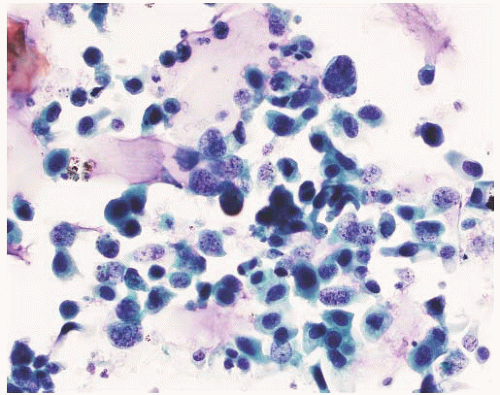 FIGURE 6-43 ▪ Bladder washing specimen from a high-grade papillary urothelial carcinoma. |
|
 FIGURE 6-44 ▪ Invasive (pT2b) high-grade urothelial carcinoma with a somewhat polypoid appearance. |
 FIGURE 6-45 ▪ Invasive (pT3b) high-grade urothelial carcinoma. |
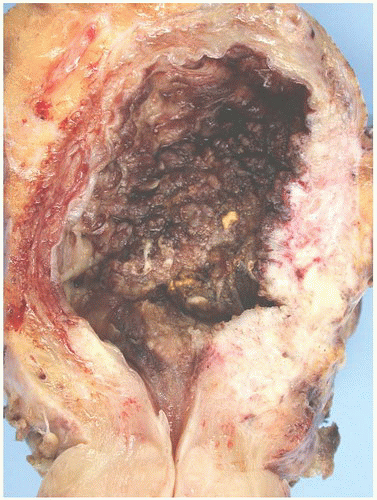 FIGURE 6-46 ▪ Invasive (pT3b) high-grade urothelial carcinoma. |
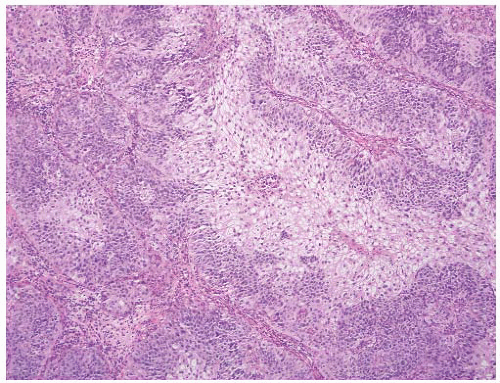 FIGURE 6-47 ▪ Invasive high-grade urothelial carcinoma growing in large nests. Note the squamoid appearance. |
|
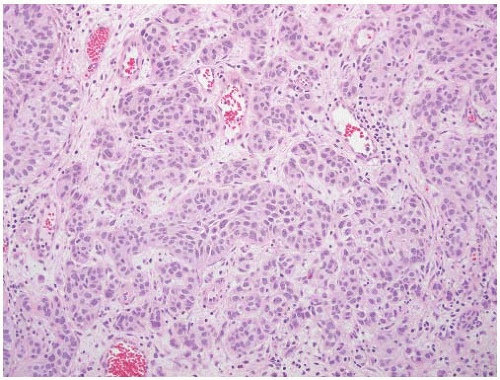 FIGURE 6-48 ▪ Invasive high-grade urothelial carcinoma with small variably shaped nests. |
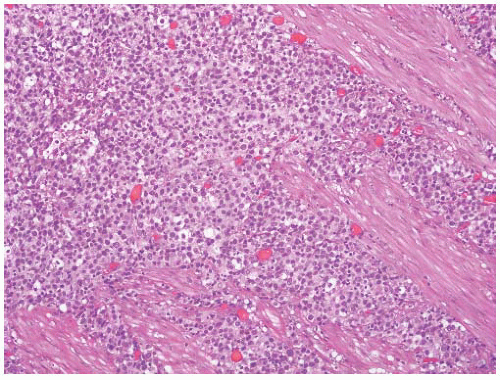 FIGURE 6-49 ▪ Invasive high-grade urothelial carcinoma growing as a solid sheet of cells. |
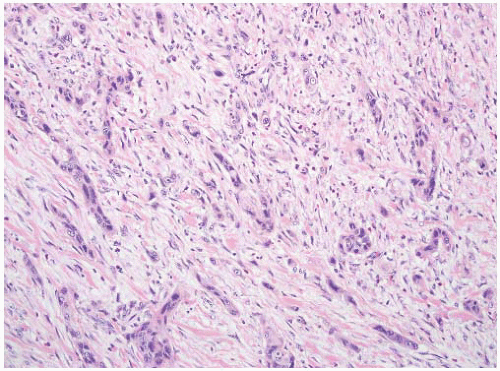 FIGURE 6-50 ▪ Invasive high-grade urothelial carcinoma forming small cords in a desmoplastic stromal background. |
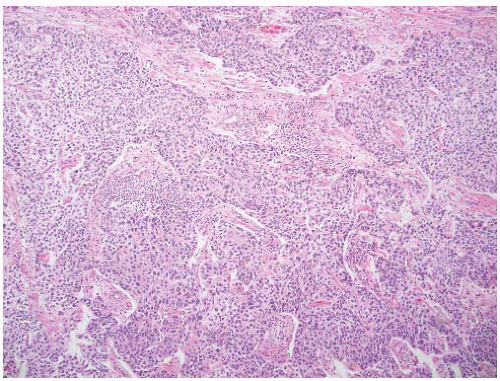 FIGURE 6-51 ▪ Invasive high-grade urothelial carcinoma with a trabecular architecture. |
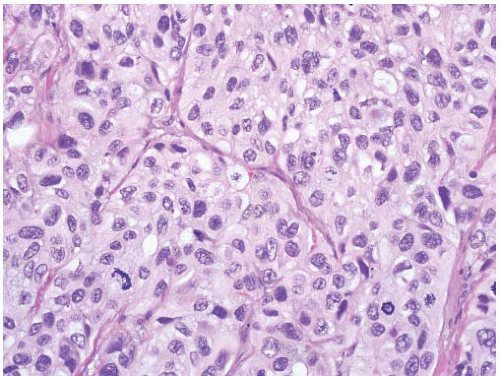 FIGURE 6-52 ▪ Invasive high-grade urothelial carcinoma with nuclear pleomorphism. |
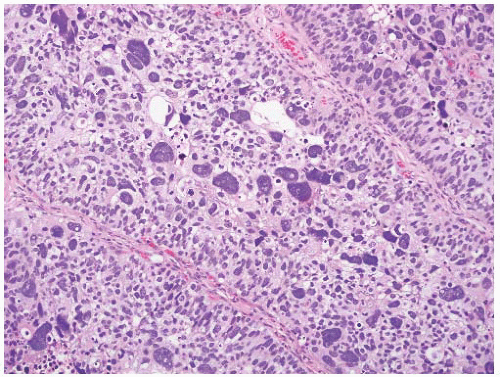 FIGURE 6-53 ▪ Invasive high-grade urothelial carcinoma with bizarre pleomorphic nuclei. |
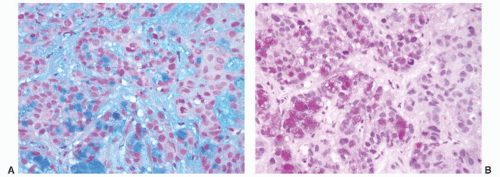 FIGURE 6-54 ▪ Mucin positivity (A, Alcian blue pH 2.4; B, mucicarmine) in an otherwise typical high-grade urothelial carcinoma. |
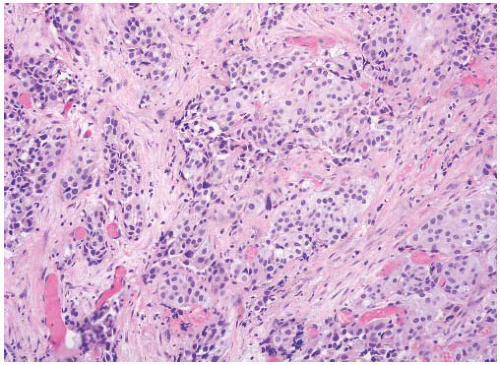 FIGURE 6-55 ▪ Invasive high-grade urothelial carcinoma with desmoplastic stroma. |
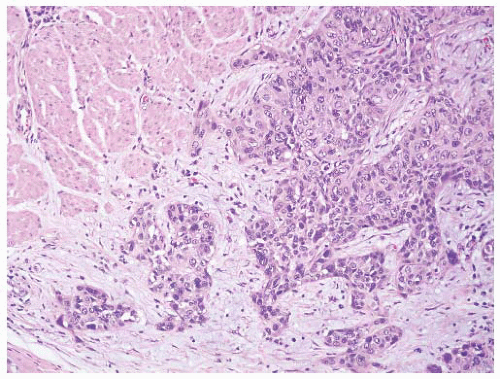 FIGURE 6-56 ▪ Invasive high-grade urothelial carcinoma with myxoid stroma. |
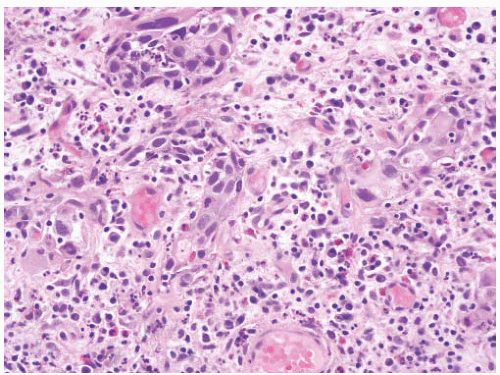 FIGURE 6-57 ▪ Invasive high-grade urothelial carcinoma with inflammation including lymphocytes, plasma cells, and eosinophils. |
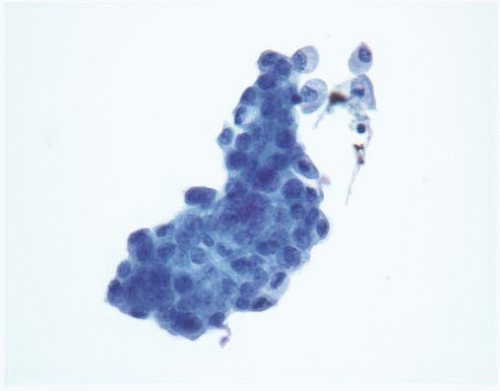 FIGURE 6-58 ▪ High-grade urothelial carcinoma in a voided urine specimen. |
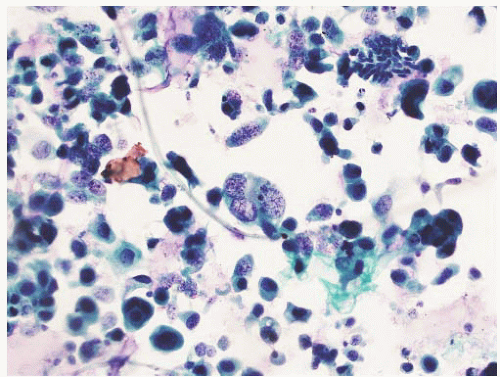 FIGURE 6-59 ▪ High-grade urothelial carcinoma in a bladder wash specimen. |
 FIGURE 6-60 ▪ High-grade urothelial carcinoma in a bladder wash specimen. |
of the bladder, lung, ovary, pancreas, and breast among others.244,254 More recently, GATA3 has been shown to be expressed in 67% of urothelial carcinomas.256 In an extensive tissue microarray study, Higgins et al.256 found only ductal adenocarcinoma of the breast to also express GATA3 indicating a high degree of specificity for this marker. These authors also reported expression of S100P in 78% of bladder urothelial carcinomas but this marker was less specific with gastrointestinal tract adenocarcinoma, hepatocellular carcinoma, ovarian carcinoma, and rarely (2%) prostatic adenocarcinoma also being positive.256
Table 6-10 ▪ IMMUNOHISTOCHEMISTRY OF UROTHELIAL CARCINOMA (USUAL TYPE) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
50% to 62%.241,242 Up to 14% of high-grade urothelial carcinomas do not express either cytokeratin 7 or 20.241,275 The results are highly dependent on case selection as cytokeratin 20 expression is much less often present in invasive and metastatic urothelial carcinomas (44%).244
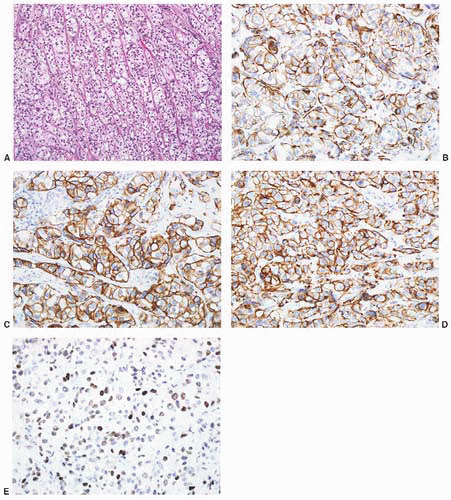 FIGURE 6-61 ▪ High-grade urothelial carcinoma with an unusual architecture (A) that has positive immunoreactivity for high molecular weight cytokeratin 34βE12 (B), cytokeratin 7 (C), cytokeratin 20 (D), and p63 (E). |
related to assisting in the differential diagnosis with prostatic adenocarcinoma242 and its expression in the spindle cell component of sarcomatoid carcinomas.
Table 6-11 ▪ VARIANTS OF UROTHELIAL CARCINOMA | ||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||
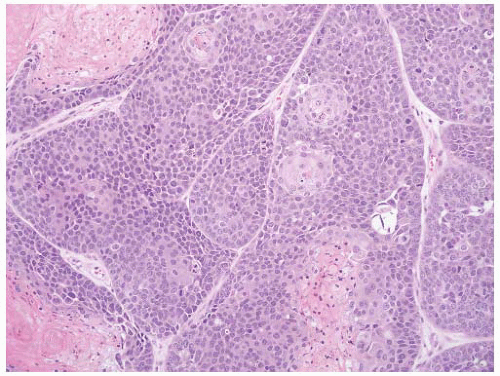 FIGURE 6-62 ▪ Urothelial carcinoma with squamous differentiation. |
with glandular differentiation, we report the percentage of the glandular component.
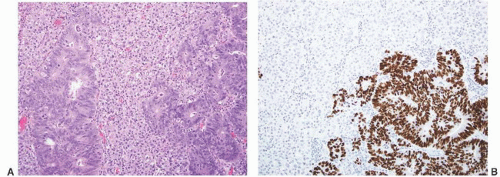 FIGURE 6-63 ▪ Urothelial carcinoma with glandular differentiation (A). The glandular component has positive immunoreactivity for CDX2 (B). |
|
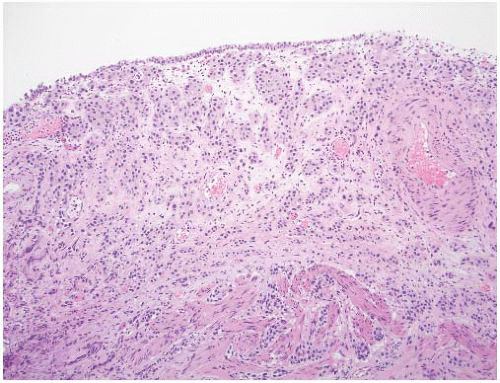 FIGURE 6-64 ▪ Nested variant of urothelial carcinoma with infiltrating small nests of cells. |
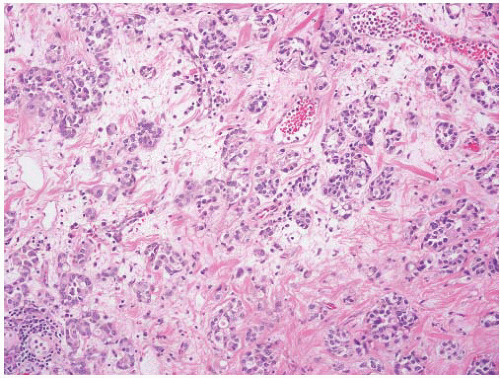 FIGURE 6-65 ▪ Nested variant of urothelial carcinoma with a more obvious high-grade component. |
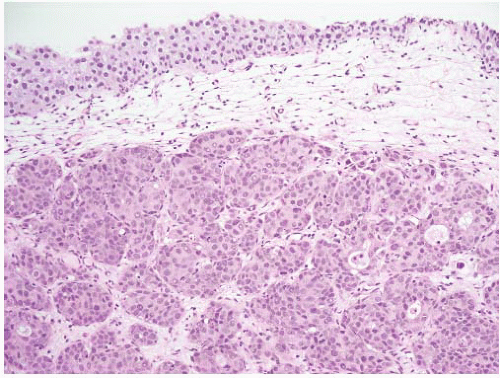 FIGURE 6-66 ▪ Nested variant of urothelial carcinoma with the nests focally becoming confluent. |
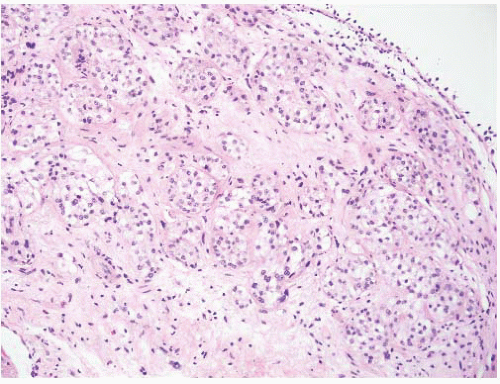 FIGURE 6-67 ▪ Nested variant of urothelial carcinoma with uniform nests and uniform round nuclei. |
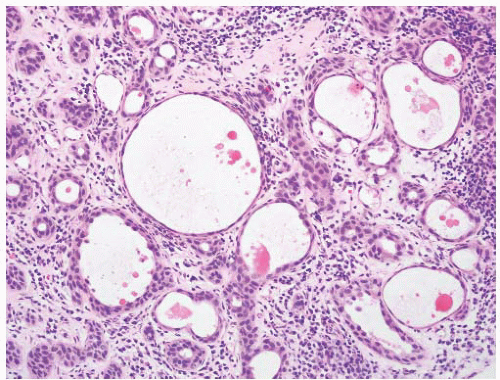 FIGURE 6-68 ▪ Microcystic variant of urothelial carcinoma with variably sized cystic spaces and some solid nests. |
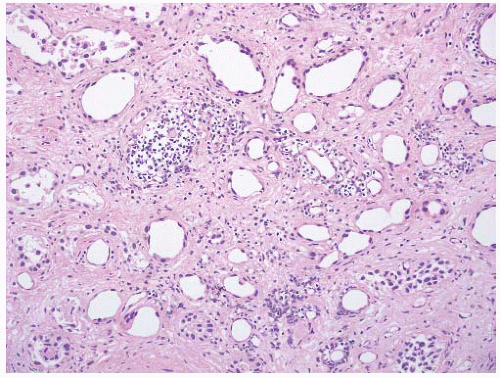 FIGURE 6-69 ▪ Microcystic variant of urothelial carcinoma with the tumor cells having scant cytoplasm producing structures that mimic lymph-vascular spaces. |
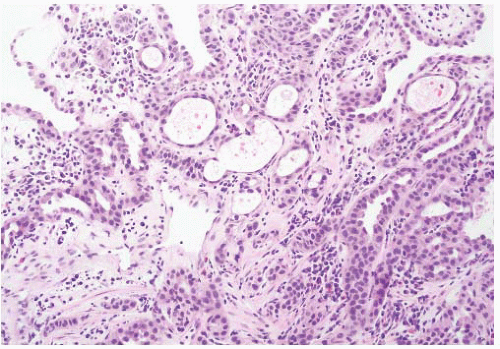 FIGURE 6-70 ▪ Urothelial carcinoma with tubule formation. This case mimics nephrogenic adenoma. |
resection specimens, a repeat resection of the area is indicated if muscle invasion is not demonstrable in the original material. Occult lymph node metastases were present in 27% of cases at the time of cystectomy in one series.311 Some authors have advocated immediate cystectomy in T1 cases.318
 FIGURE 6-71 ▪ Micropapillary variant of urothelial carcinoma. The tumor in this case was 90% micropapillary. |
|
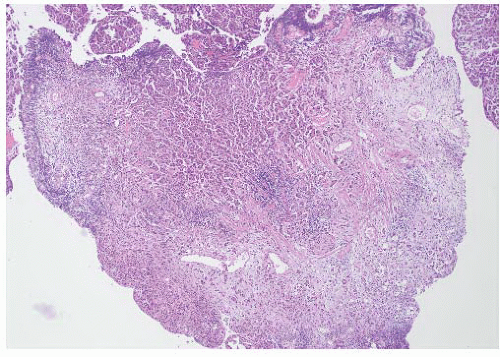 FIGURE 6-72 ▪ Micropapillary variant of urothelial carcinoma in a TURBT chip. |
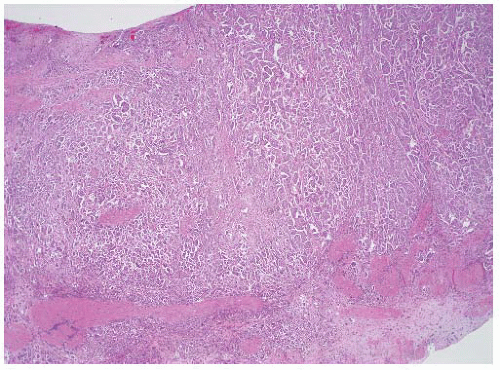 FIGURE 6-73 ▪ Micropapillary variant of urothelial carcinoma in a section from a cystectomy specimen. |
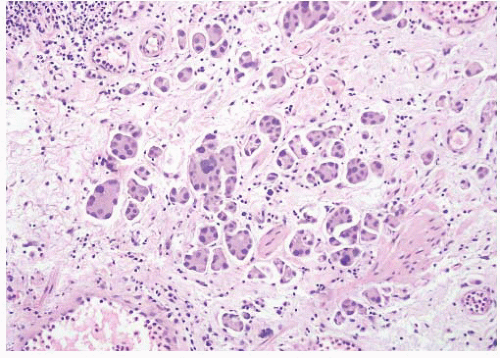 FIGURE 6-74 ▪ Micropapillary variant of urothelial carcinoma in the lamina propria. |
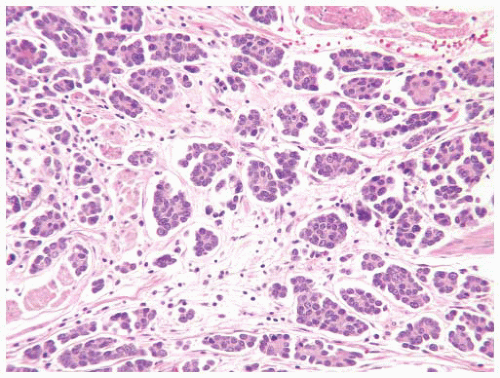 FIGURE 6-75 ▪ Micropapillary variant of urothelial carcinoma with prominent peripheral location of nuclei. |
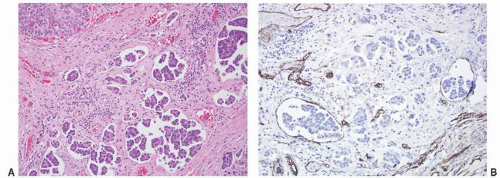 FIGURE 6-76 ▪ Micropapillary variant of urothelial carcinoma (A) with some of the nests in spaces lined by CD34-positive cells (B). Note the usual urothelial carcinoma component in the upper left. |
 FIGURE 6-77 ▪ Micropapillary variant of urothelial carcinoma involving a ureter resection margin (the surgeon could not get a clear margin in this case). |
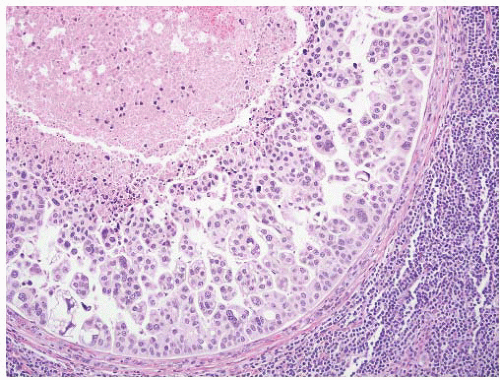 FIGURE 6-78 ▪ Micropapillary variant of urothelial carcinoma metastatic to a pelvic lymph node. |
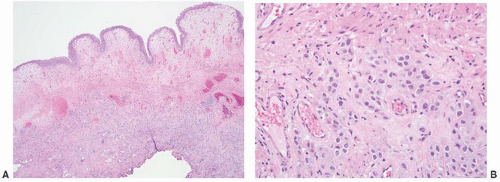 FIGURE 6-79 ▪ Plasmacytoid variant of urothelial carcinoma in a TURBT specimen. The mucosa is edematous (A) with the tumor cells in the deep lamina propria (B). |
cells are medium sized with pale eosinophilic cytoplasm and eccentric nuclei producing the plasmacytoid appearance (Fig. 6-80). The appearance can be strikingly plasma cell-like such that plasmacytoma is strongly considered in the differential diagnosis.334 In some cases, the cytoplasm is more basophilic. Many cells have an area of perinuclear clearing that may be mucin positive. In all cases, a minority of cells have true signet ring morphology. The nuclei tend to be round or indented with prominent nucleoli in a minority. Overall there is a more uniform nuclear appearance than typical of urothelial carcinoma (Fig. 6-81). The cells tend to infiltrate as single cells (Fig. 6-82) or cords of cells but can also form nests and sheets (Fig. 6-83). The diffusely permeative nature results in the tumor being more extensive than appreciated clinically or on gross examination. These can be extremely challenging at frozen section evaluation of ureter margins, and knowledge of the histology is very helpful in avoiding false-negative interpretations. Typical urothelial carcinoma, often a surface papillary carcinoma, is present in the majority of cases. The diagnosis of carcinoma can be confirmed by positive immunoreactivity for cytokeratin, EMA, and CEA with negative reactivity for lymphoid markers.
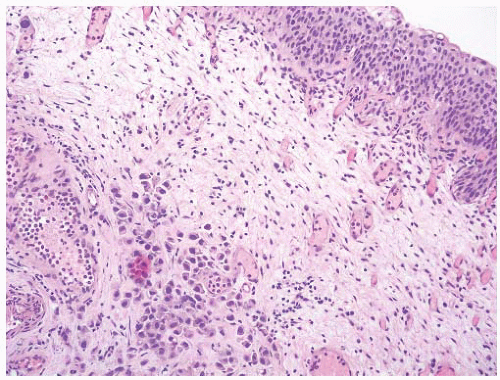 FIGURE 6-80 ▪ Plasmacytoid variant of urothelial carcinoma in the lamina propria. |
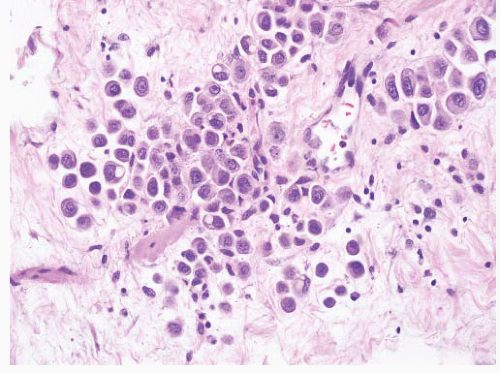 FIGURE 6-81 ▪ Plasmacytoid variant of urothelial carcinoma illustrating the morphologic range of the individual cells. A few tumor cells have cytoplasmic vacuoles. |
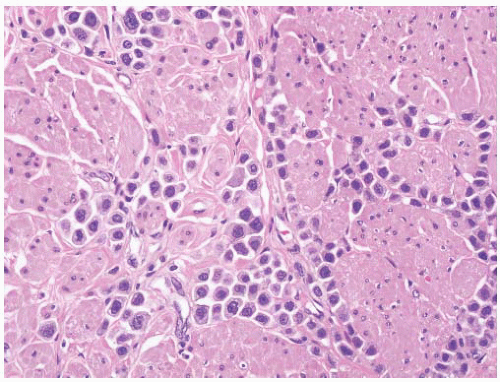 FIGURE 6-82 ▪ Plasmacytoid variant of urothelial carcinoma infiltrating between smooth muscle bundles of the muscularis propria. |
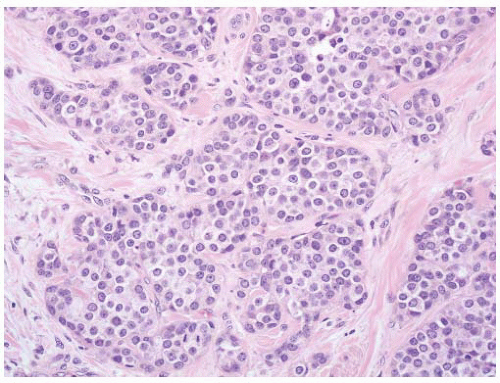 FIGURE 6-83 ▪ Plasmacytoid variant of urothelial carcinoma with the cells forming more defined nests. |
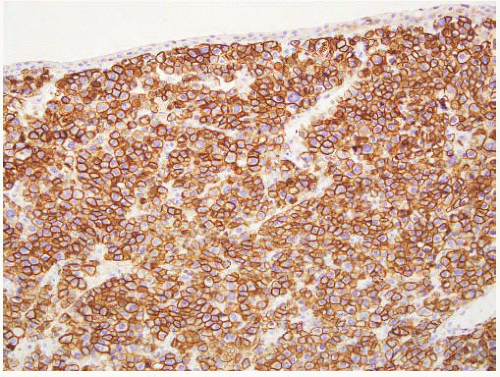 FIGURE 6-84 ▪ Plasmacytoid variant of urothelial carcinoma with strong immunoreactivity for CD138. |
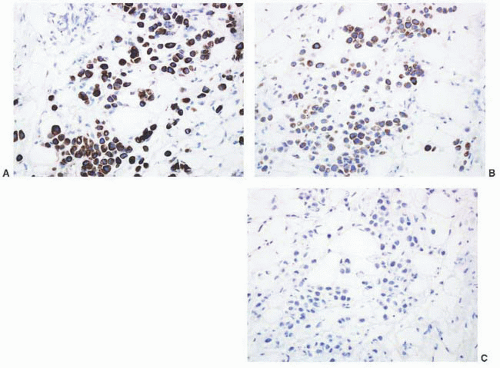 FIGURE 6-85 ▪ Plasmacytoid variant of urothelial carcinoma with positive immunoreactivity for cytokeratins 7 (A) and 20 (B) but not for p63 (C). |
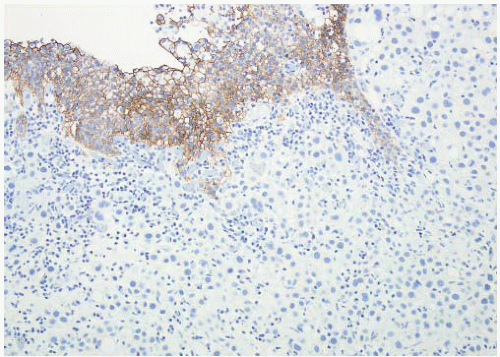 FIGURE 6-86 ▪ Plasmacytoid variant of urothelial carcinoma with loss of expression of E-cadherin. |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


