iliac nodes. The sympathetic nerves that innervate the bladder are derived from the T11-L2 nerve roots; these sympathetic nerves play no role in micturition. The parasympathetic nerves originate from the S2-S4 roots and travel to the bladder via the pelvic nerve and inferior hypogastric plexus. These peripheral nerves cause contraction of the muscularis propria fibers, which leads to traction of the bladder, opening of the internal sphincter, and emptying of urine into the urethra.
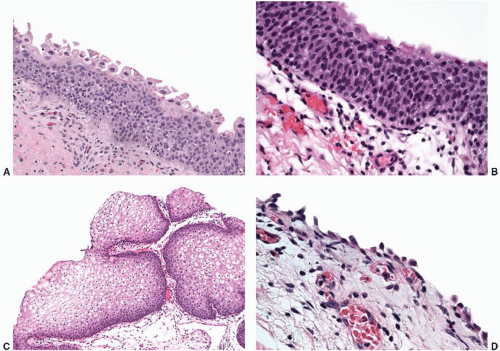 FIGURE 5-1 ▪ A: Normal urothelium may have a prominent umbrella cell layer. These cells may have enlarged nuclei with multilobulation and cytoplasmic vacuolization. These features should not be regarded as neoplastic. B: In general, normal urothelium shows a streaming arrangement of the urothelial cells arranged perpendicular to the basement membrane. The urothelial cells often have nuclear grooves along the long axis of the cell. C: In the trigone of women, the surface lining is often composed of a glycogenated nonkeratinizing squamous epithelium. D: In biopsy specimens, particularly those performed with “hot” loops, denudation of the surface urothelium is not uncommon. Scattered residual benign basal cells may be present. |
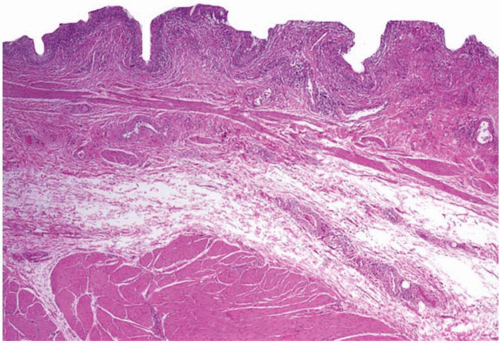 FIGURE 5-2 ▪ The lamina propria is defined as the tissue between the urothelium and the muscularis propria. It often contains disorganized wispy fascicles of smooth muscle called the muscularis mucosae, as well as loose stroma and varying caliber blood vessels. |
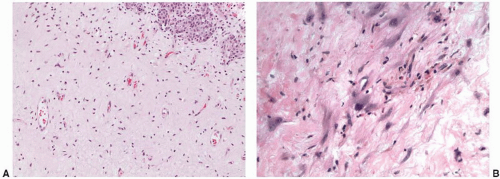 FIGURE 5-3 ▪ A: The stroma within the lamina propria may be edematous or finely collagenized, as in this example. The majority of the stroma cells are small and inconspicuous. B: However, scattered stromal cells with enlarged hyperchromatic or multilobated nuclei are not uncommon, and (C) these stromal cells may be numerous. D: Varying caliber blood vessels set in a fine stroma are also characteristic of the lamina propria. |
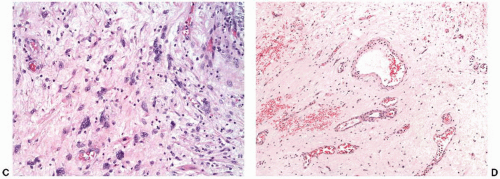 FIGURE 5-3 ▪ (Continued) |
and adipose tissue (Fig. 5-6A).5,6 Although the muscularis mucosae may have individual thick muscle bundles (i.e., hyperplastic muscularis mucosae), the muscularis propria has distinct tight aggregates of several discernable compact smooth muscle bundles that aid in their recognition (Fig. 5-6B). Because of variation in thickness of the lamina propria, the muscularis propria may be surprisingly superficial in some biopsies, particularly in the trigone (Fig. 5-6C). In this location, typical deeper muscularis propria bundles become smaller in caliber as they reach toward the surface and are found in almost a suburothelial location.
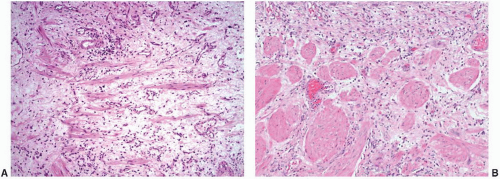 FIGURE 5-4 ▪ A: The histology of the muscularis mucosae is classically described as disorganized wispy fascicles of smooth muscle within the lamina propria. B: However, recent studies have described more histologic variability. In the dome, individual rounded bundles of smooth muscle are common. C: Unlike muscularis propria, these individual rounded bundles of muscularis mucosae are separated by stroma. D: In patients with urinary outlet obstruction, typically due to prostatic hyperplasia, the muscularis mucosae may become hypertrophic. The disarray of the smooth muscle fibers characterizes hyperplastic muscularis mucosae. |
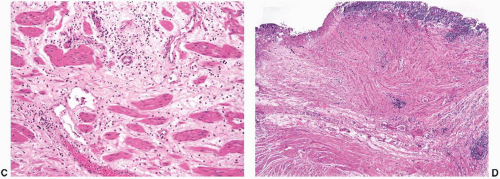 FIGURE 5-4 ▪ (Continued) |
Table 5-1 ▪ MUSCULARIS MUCOSAE VERSUS MUSCULARIS PROPRIA | ||||
|---|---|---|---|---|
|
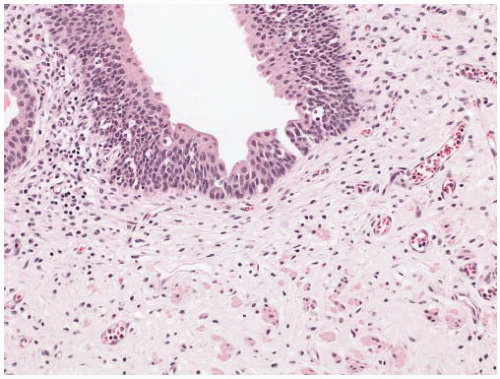 FIGURE 5-5 ▪ There is a variably cellular layer of spindled myofibroblasts beneath the urothelium. These cells often show elongated nuclei and long cytoplasmic processes. |
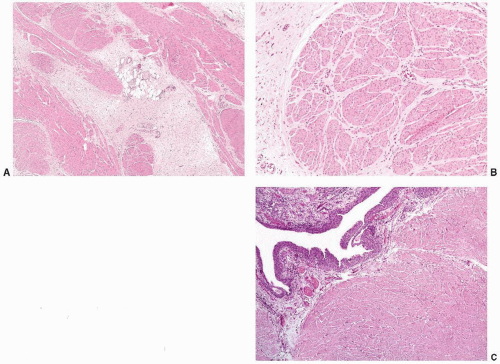 FIGURE 5-6 ▪ A: Adipose tissue may be present at any level within the bladder wall. In this example, a lobule of adipose tissue is seen within the muscularis propria. B: The muscularis propria is comprised of compact well-delineated aggregates of smooth muscle. C: In some areas, such as the trigone, the muscularis propria is located very superficially. |
agenesis or other abnormalities that lead to an absence of urine entering the bladder (e.g., bilateral ureteral ectopia).30 Rarely, bladder hypoplasia may be due to an absence of urine collection in the bladder due to low outlet resistance from causes such as epispadias.
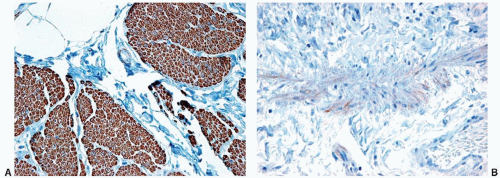 FIGURE 5-7 ▪ Antismoothelin antibodies highlight the muscularis propria (A) with a strong and diffuse pattern of immunoreactivity. In contrast, the muscularis mucosae (B) are typically negative or show only weak, focal staining. |
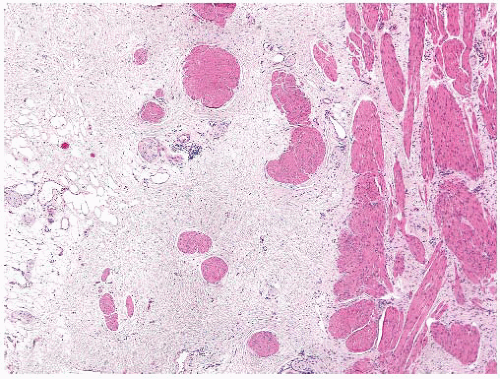 FIGURE 5-8 ▪ The interface between the muscularis propria and the perivesical soft tissue is often irregular, which may cause difficulties in assessing microscopic invasion for staging purposes. |
two bladders with fully formed mucosal and muscular walls. Each side receives a single ureter and drains into separate duplicate urethras. Complete duplication is typically associated with duplication of the internal and external genital organs, hindgut, and caudal vertebral column.36 Partial duplication, which is less common than the complete form, is defined as two bladders that share a common bladder neck and drain into a common urethra.
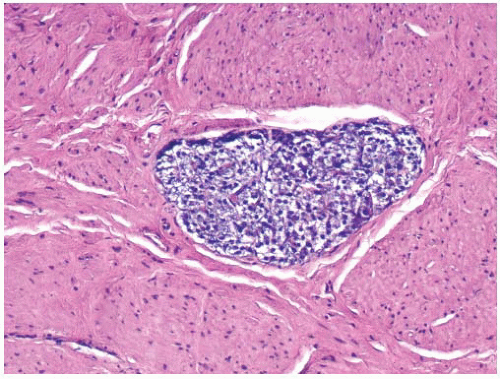 FIGURE 5-9 ▪ Incidental paraganglia may rarely be found in the bladder wall. These are likely the origin of rare bladder paragangliomas. |
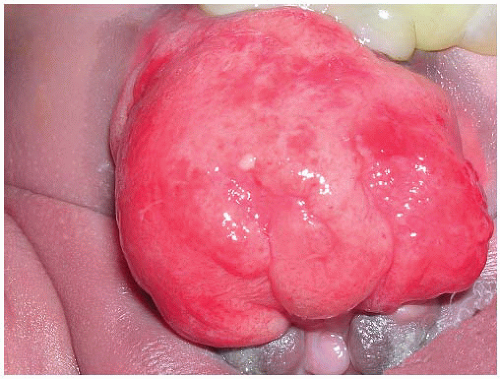 FIGURE 5-10 ▪ Bladder exstrophy is clinically striking with the bladder mucosa exposed on the surface of the abdominal wall. (Courtesy: Dr. Michael Hsieh, Stanford University.) |
Some are associated with syndromes such as Klippel-Trenaunay-Weber syndrome.58,59 Preoperative imaging often suggests a vascular lesion, and in large masses Doppler flow studies may show a shunt in lesions with an arterial component. Morphologically, these lesions consist of large abnormally dilated vascular channels with varying components of arterial, venous, and lymphatic vessels (Fig. 5-11). The vessel walls vary in thickness with varying amounts of medial and elastic layers. Vascular malformations may have overlying ulceration and associated reactive urothelial atypia, including pseudosarcomatous epithelial hyperplasia.60
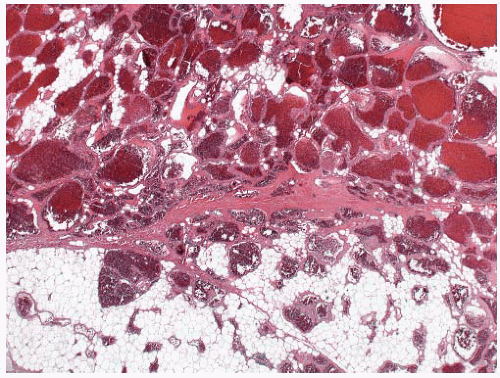 FIGURE 5-11 ▪ Vascular malformations are typically comprised of dilated vascular spaces admixed with fat or normal bladder tissues. |
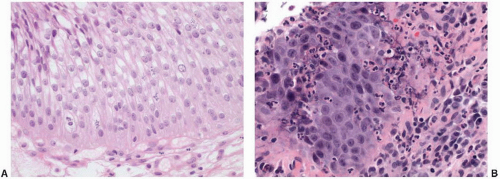 FIGURE 5-12 ▪ A: This example of reactive urothelial atypia is associated with an indwelling catheter. Nuclear enlargement and small nucleoli are typical in reactive urothelial changes. In contrast to flat neoplasia, the nuclear contours are sharp and the chromatin remains fine and evenly distributed. Mitotic figures may be increased and may extend into the upper layers of the urothelium. B: In this example of reactive atypia, the nucleoli are more prominent, but the chromatin remains fine. Neutrophilic infiltrates are also common. |
some cases, usually with recent catheterization, papillary/polypoid cystitis shows marked reactive epithelial changes with small, prominent nucleoli, urothelial hyperplasia, and mitotic activity mimicking a high-grade lesion.70 In general, papillomas have more slender papillae; the papillae of papillary cystitis often have a bulbous tip with prominent stromal edema. In addition, urothelial papillomas have other features that, at least in aggregate, may aid in the distinction when present: a very prominent umbrella cell layer or marked cytoplasmic vacuolization, a gland-in-gland pattern within the papillae, a dilated lymphatic space filling the papillae, a more complex papillary pattern with secondary and tertiary branching, and an admixed endophytic (inverted) component.71,72 Significant cytologic atypia within a papillary lesion or the adjacent urothelium favors a diagnosis of neoplasia.
Table 5-2 ▪ IMMUNOPHENOTYPE OF FLAT LESIONS | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
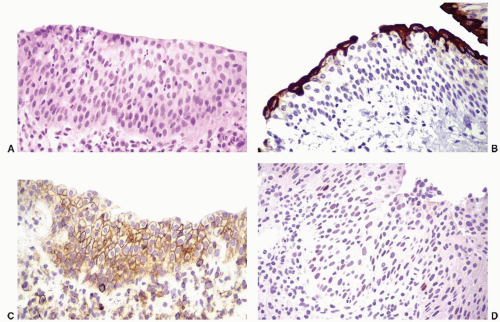 FIGURE 5-13 ▪ Reactive urothelial atypia (A, H&E) has a characteristic immunophenotype with CK20, CD44, and p53 immunohistochemistry. CK20 (B) highlights the umbrella cell layer, while CD44 (C) shows strong membranous reactivity in the full thickness of the urothelial cells. p53 (D) shows weak and isolated nuclear staining, but strong and diffuse reactivity is not seen. |
| ||||||||||||||||||||||
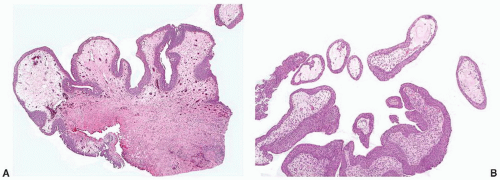 FIGURE 5-14 ▪ A: In papillary/polypoid cystitis, the exophytic projections have a broad base due to underlying edema. In addition, the complex hierarchical branching of papillary neoplasia is absent. B: Biopsies taken near the tips of the papillary component may easily be mistaken for papillary neoplasia. |
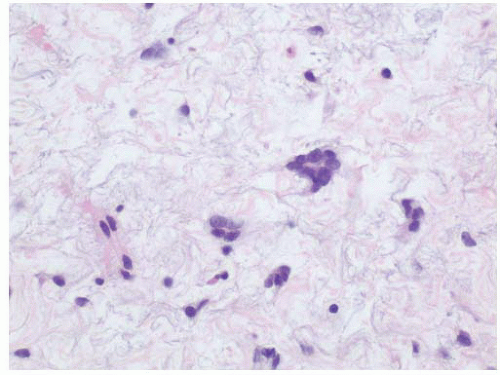 FIGURE 5-15 ▪ Increased numbers of multinucleated atypical stromal cells within the lamina propria have been termed giant-cell cystitis. |
known bladder irritants, concomitant urothelial neoplasia, and infections would exclude the diagnosis of interstitial cystitis.81 The American Urologic Association guidelines have provided the following modified definition: “An unpleasant sensation (pain, pressure, discomfort) perceived to be related to the urinary bladder, associated with lower urinary tract symptoms of more than 6 weeks duration, in the absence of infection or other identifiable causes.”83
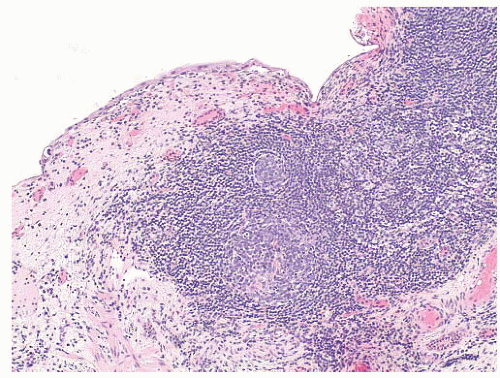 FIGURE 5-16 ▪ Follicular cystitis is characterized by mature lymphocytic infiltrates with germinal center formation. |
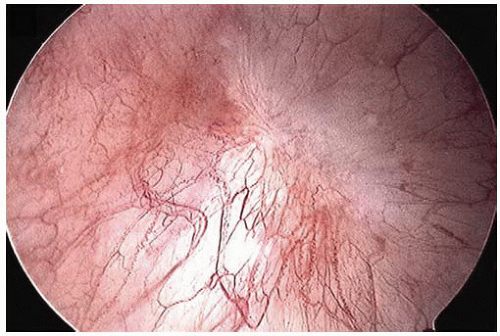 FIGURE 5-17 ▪ Interstitial cystitis is often characterized cystoscopically by small foci of mucosal hemorrhage called glomerulations. |
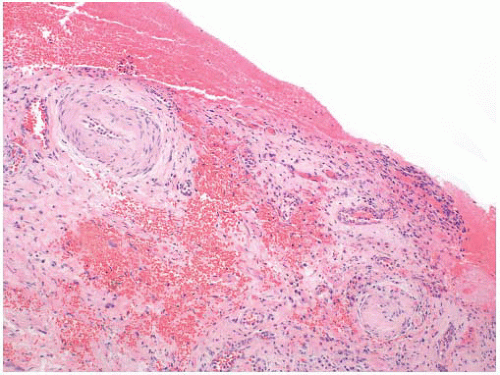 FIGURE 5-18 ▪ In interstitial cystitis, variable surface erosion with hemorrhage is common. |
toxicity may be potentiated by concomitant therapy with cyclophosphamide. Radiation-induced histologic changes are similar to those seen with intravesical chemotherapy, but with intravesical chemotherapy the histologic changes are often more restricted to the superficial urothelial cell layer. Atypical mesenchymal cells similar to those seen in giantcell cystitis are also typically present in the lamina propria (Fig. 5-21). Other characteristic changes of radiation injury including marked stromal edema or fibrosis; prominent telangiectatic change, hyalinization, and thrombosis of the vessels are also helpful. Pseudocarcinomatous hyperplasia of the epithelium (discussed later) may be striking.
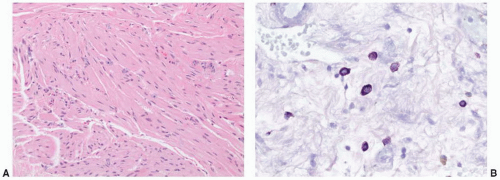 FIGURE 5-19 ▪ A: Although its specificity has been debated, increased mast cells within the muscularis propria are reported in interstitial cystitis. B: The mast cells may be highlighted by a toluidine blue stain. |
uniformly eosinophilic, and nuclear changes similar to those seen with radiation are common (Fig. 5-22A and B).
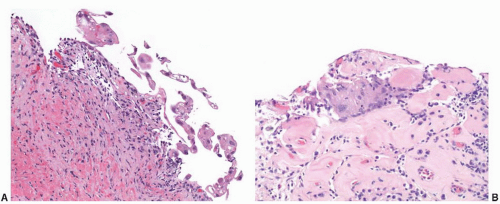 FIGURE 5-20 ▪ A: Urothelial atypia secondary to radiation therapy is generally characterized by nuclear enlargement, prominent cytoplasmic vacuolization, and (B) multinucleation. The underlying tissue, including blood vessels, commonly shows hyalinization. |
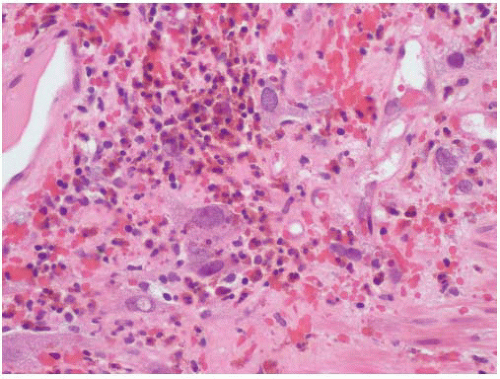 FIGURE 5-21 ▪ With radiation therapy, the stromal cells of the bladder may suggest prior radiation exposure given the degree of atypia with marked variation in size. |
young adults; however, it should be emphasized that there is no relationship to Langerhans cell histiocytosis (previously called eosinophilic granuloma).
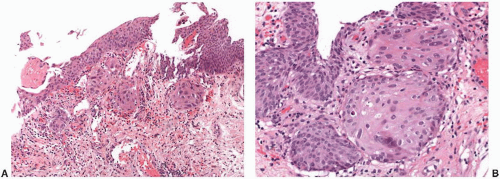 FIGURE 5-22 ▪ A: After intravesical chemotherapy, nests of urothelial cells with atypical features may underlie a relatively normal appearing re-epithelialized urothelium. These reactive cells have enlarged nuclei and commonly have more eosinophilic cytoplasm imparting a squamoid appearance. B: At higher magnification, the fine chromatin of the reactive urothelial cells with enlarged nuclei can be seen. Compared to the overlying urothelium, these nests of cells with prior exposure to intravesical chemotherapy have a more pronounced cytoplasmic eosinophilia. |
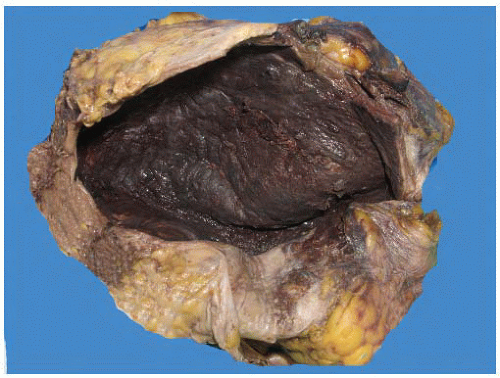 FIGURE 5-23 ▪ In this postmortem bladder specimen, the diffuse mucosal hemorrhage characteristic of hemorrhagic cystitis due to prior systemic chemotherapy is seen. (Courtesy: Dr. Don Regula, Stanford University.) |
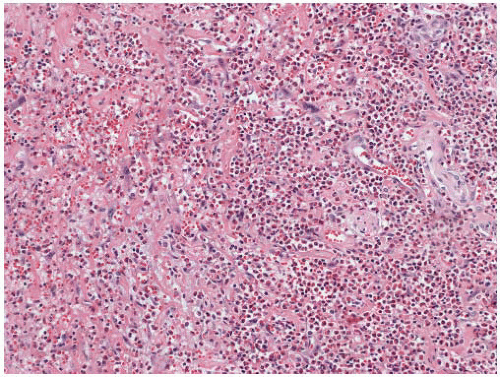 FIGURE 5-24 ▪ Although nonspecific, the extensive infiltrates of eosinophils typical of eosinophilic cystitis are seen in this biopsy specimen from a bladder mass in a child. |
bladder. This lesion is typically associated with bacterial infections such as E. coli or Aerobacter zaerogenes. In adults, an association with diabetes/hyperglycemia is described in up to 50% of cases, but it may also be seen in association with neurogenic bladder, chronic cystitis, or immunosuppressed states.105,106
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


