Fig. 4.1
Positioning the patient in lithotomy position allows for a member of the surgical team to stand between the patient’s legs. Hip flexion is minimal to avoid interference between the thighs and the instruments while working in the upper abdomen. This patient is secured to the table with a beanbag and tape to allow for extremes of table positioning
Fig. 4.2
This schematic drawing depicts the positioning of the operating team and monitor during a laparoscopic colectomy. The first assistant can stand between the patient’s legs
The camera port should be placed in the center of the abdomen through a periumbilical incision centered between the patient’s pubic synthesis and the xiphoid process at the top of the dome of the insufflated abdomen. Additionally, two or three other working ports are usually necessary to perform this operation. Generally, the umbilical camera incision can be extended and used as the extraction site. Two alternatives for placing the working ports are illustrated in Figs. 4.3 and 4.4.
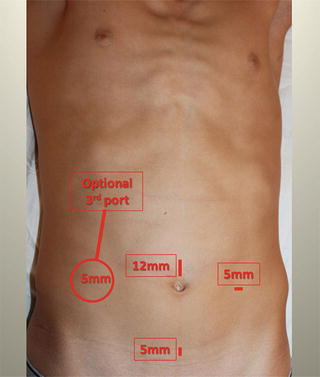
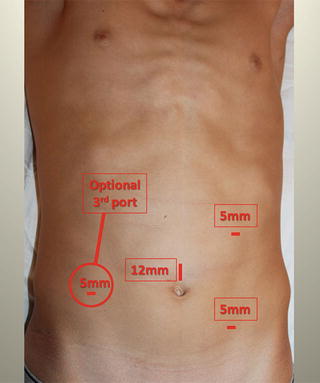
Figs. 4.3 and 4.4
Two alternative port positions for a laparoscopic right colectomy. A third working port can be added in the right lower quadrant if needed
Clinical Anatomy
The right colon and its mesentery are intimately associated with the retroperitoneum in the right abdomen. It is suspended laterally by peritoneal attachments to the abdominal wall. The hepatic flexure has attachments to the posterior diaphragm and undersurface of the liver and gallbladder. Moving distally along the transverse colon, the colon fuses with the omentum and is attached to the greater curve of the stomach by the gastrocolic omentum. The superior aspect of the proximal transverse colon mesentery has avascular attachments to the posterior wall of the stomach. Proceeding distally along the transverse colon mesentery, the lesser sac forms the superior border. The blood supply to the right colon consists of the ileocolic vessels and, variably, the right colic or right braches of the middle colic vessels.
The retroperitoneal boundaries of the right colon and its mesentery form a triangle extending from the fourth portion of the duodenum inferolaterally to the cecum, up the right colic gutter, and then medially from the hepatic flexure to the middle colic vessels. The retroperitoneal attachments of the right colon are avascular. Within this retroperitoneal triangle posterior to the right colon, the right gonadal vessels are encountered first, moving from lateral to medial. The next vertically oriented structure is the right ureter, which crosses over the right common iliac vessels at the inferomedial border of this triangle. The vena cava is the next structure medial to the ureter running vertically in this plane. Proceeding cephalad in this plane, the second and third portions of the duodenum and head of the pancreas are encountered next. Just medial to the pancreatic head, the middle colic vessels are encountered. Lateral to these structures, the hepatic flexure lies over Gerota’s fascia of the right kidney.
Objectives of the Laparoscopic Procedure
Four objectives must be accomplished in order to complete a laparoscopic right colectomy: (1) the right colon and its mesentery must be mobilized off of the retroperitoneum and duodenum; (2) the vascular pedicles must be divided at the appropriate level for the disease process; (3) the lateral attachments, hepatic flexure, and omental attachments must all be divided; and (4) the specimen must be extracted and the anastomosis performed.
There are four commonly used approaches for a laparoscopic right colectomy—the medial, inferior, lateral, and superior approaches. Regardless of the method, the purpose is to mobilize the right colon completely from the retroperitoneum and the sweep of the duodenum. This accomplishes three purposes—it allows for safe ligation of the mesenteric vessels; it frees the colon so that it can be delivered out through the extraction site; and lastly, it allows for a tension-free ileocolic anastomosis.
Medial Approach
The medial approach to the right colectomy involves an initial incision through the ileocolic mesentery underneath the ileocolic artery (Video 4.1). This vascular pedicle is identified by grasping the cecal mesentery and lifting it anteriorly down into the right lower quadrant. The vessels will form a bowstring in the mesentery. The peritoneum below the vessel is incised, and the retroperitoneal plane is identified. The initial retroperitoneal dissection is performed bluntly through this window. The duodenum is encountered early in the dissection and should be gently swept down from the mesentery. Once the duodenum has been identified and is safely dissected away from the pedicle, the ileocolic artery can be divided. Vascular ligation allows this window to be opened widely and greatly facilitates the remainder of the retroperitoneal dissection. Gentle blunt dissection should be carried out in this plane laterally beyond the colon and in a cephalad direction beyond the hepatic flexure. The entire sweep of the duodenum should be swept down in order to complete the mobilization.
Inferior Approach
The inferior approach begins with a peritoneal incision underneath the terminal ileal mesentery extending from the distal mesentery up to the duodenum. As in the medial approach, the retroperitoneal dissection also proceeds superiorly and laterally. An advantage of this approach is that the window aperture is much wider than with the medial approach. The duodenum is again identified in the retroperitoneum and swept out of harm’s way. This dissection should continue laterally beyond the colon and in a cephalad direction beyond the hepatic flexure, again including the entire sweep of the duodenum.
Lateral Approach
The lateral approach is similar to the conventional open approach. An advantage of this approach is that it is more familiar for a traditional open surgeon and can ease the transition to performing laparoscopic colectomies. Additionally, this approach may be necessary when inflammation or adhesions preclude the medial or inferior approach. The disadvantage of this approach is that it can sometimes be difficult to perform the retroperitoneal dissection toward the operator and the camera. Again, the duodenum should be identified in the retroperitoneum and kept safe from harm.
Superior Approach
The final approach is the superior-to-inferior approach. This approach is begun by incising the gastrocolic omentum and dissecting from medial to lateral in the plane cephalad to the mesentery of the proximal transverse colon. Dissection then proceeds inferiorly after the hepatic flexure attachments have been divided. The duodenum should be identified in the retroperitoneum as the hepatic flexure of the colon is mobilized and pulled down toward the patient’s left hip. As with the lateral approach, it becomes more difficult as the dissection proceeds medially. The superior approach is invaluable in situations in which there is a large cecal mass or significant inflammation in the right lower quadrant or the ileocolic mesentery.
Every surgeon should be familiar with all of these approaches, as different patient habitus, anatomic variation, and disease presentation often necessitates some combination of these approaches in order to adequately mobilize the colon.
The Procedure
For the purposes of this textbook, the operation will be described using the inferior approach. The other approaches will be referenced when appropriate.
After pneumoperitoneum has been established, the abdominal cavity should be visualized, and any abnormalities should be noted. If the resection is being performed for neoplastic disease, the liver should be closely inspected for metastatic disease. If a suspicious lesion is identified, it can usually be biopsied laparoscopically by passing a core needle biopsy device subcostally through a stab incision. If the resection is being performed for Crohn’s disease, the small bowel should be visualized in its entirety.
The patient should then be placed in steep Trendelenburg and in the left lateral decubitus position. As described above, it is important to secure the patient to the table in order to avoid any mishaps. The omentum should be rolled over the top of the transverse colon and draped onto the stomach. This maneuver exposes the serosal surface of the transverse colon, keeps the omentum from displacing small bowel into your field of view, and allows access to the omental attachments of the transverse colon. Next, the small bowel is swept out of the pelvis into the left upper abdomen. The terminal ileum should then be placed alongside the ascending colon, exposing the inferomedial aspect of the terminal ileal mesentery. These steps are greatly aided by the gravity resulting from proper bed positioning.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


