Fig. 13.1
Proper patient positioning in the operating room. The patient is positioned on the operating table in the supine position. The patient’s upper extremities are tucked at the side
En Bloc Jejunal/Ileal Resection
Exploratory laparotomy is performed through a midline incision. A thorough exploration of the abdomen is imperative to identify any evidence of metastatic disease. Attention should be specifically placed on examining common locations of metastatic disease including the peritoneum, liver, and omentum. The entirety of the small bowel is then examined starting at the ligament of Treitz through the end of the ileum. The area of malignancy is identified and appropriate margins are determined both proximally and distally. The mesentery adjacent to the primary tumor should be palpated for clinically positive lymph nodes, which must be included in the resected specimen. A small window in the adjacent mesentery is created for stapler placement by blunt or electrocautery dissection. The small bowel is then divided with a linear gastrointestinal anastomosis (GIA) stapling device (Ethicon Endosurgery, Cincinnati, OH). Staple selection is critical and for standard small bowel the staples should have a closed staple height of 1.5 mm (blue load). The mesentery is then divided serially using a clamp and tie technique. Two large Kelly clamps compress the mesentery, which is then sharply divided. The divided portions of mesentery are ligated using 2–0 silk sutures. Energy devices, including ultrasonic vibration instruments such as the HARMONIC FOCUS (Ethicon, Cincinnati, OH) or advanced bipolar devices such as the ENSEAL G2 (Ethicon, Cincinnati, OH), can alternatively be used to divide and ligate the mesentery. This resection is performed to the root of the mesentery with extreme caution to avoid ligation of the superior mesentery artery or one of its main branches supplying the remainder of small bowel. The entire specimen is removed en bloc and prepared for pathologic evaluation. Proximal and distal portions of small bowel are marked using silk suture. Bowel continuity is achieved through an isoperistaltic side-to-side anastomosis. This anastomosis can be performed through one of two techniques: hand-sewn technique or stapled anastomosis technique.
Hand-Sewn Anastomosis
The first step in utilizing a hand-sewn technique is to align the divided ends of small bowel in an isoperistaltic manner and secure this position by placing anchoring sutures in the mesenteric portion of the serosa. A two-layered technique is utilized. The posterior outer layer is performed first using 3–0 interrupted silk sutures. These sutures should align the two bowel segments for a distance of at least 5–6 cm. Full-thickness enterotomies are made in both of the bowel segments just above the posterior layer (Fig. 13.2a). Next, the inner layer of the two-layer anastomosis is performed as continuous running suture. This inner layer is best completed with a double-armed 3–0 absorbable suture (e.g., Maxon polyglyconate, monofilament synthetic absorbable suture, Covidien, Mansfield, MA) secured initially in the middle of the posterior inner row with full-thickness bites of each bowel segment. Continual full-thickness bites are taken as the running suture continues to each corner of the anastomosis (Fig. 13.2b). This continuous suture is continued on the anterior portion of the anastomosis and secured in the middle of the anterior row completing the inner layer of the anastomosis (Fig. 13.2c). Next, the anterior portion of the outer layer is completed with interrupted, seromuscular bites placed in Lembert fashion using 3–0 silk suture (Fig. 13.2d). The mesenteric defect is closed with interrupted silk sutures to prevent internal herniation.
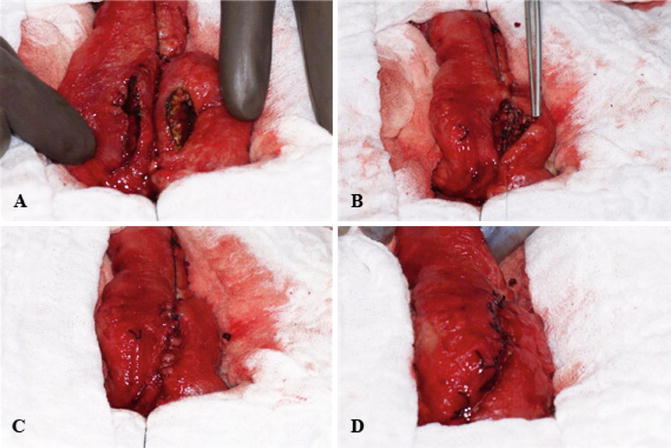
Fig. 13.2
Hand-sewn anastomosis. (a) Full-thickness enterotomies are made for a distance of 5–6 cm. (b) The inner layer of the anastomosis is performed with a continuous running suture. This layer is initiated on the posterior aspect of the anastomosis and progresses (c) to include entire circumference of the enterotomies. (d) The anastomosis is completed with anterior seromuscular sutures
Stapled Anastomosis
Similarly, the divided ends of the small bowel are aligned in an isoperistaltic manner. Serosal anchoring sutures are placed in the mesenteric side of the bowel serosa ensuring proper alignment of the divided ends (Fig. 13.3a). Full-thickness enterotomies are made on the antimesenteric surface of both divided ends approximately 1 cm distal to the staple lines (Fig. 13.3b). Side-to-side enteroenterostomy is created along the antimesenteric portion of the divided bowel using a linear GIA stapling device with 3.8 mm staple load (1.5 mm closed staple height) (Fig. 13.3c). The remaining bowel defect is then closed with interrupted, 3–0 silk sutures placed in Lembert fashion (Fig. 13.3d). The mesenteric defect is again closed with simple, interrupted sutures (2–0 silk) to prevent future internal herniation.
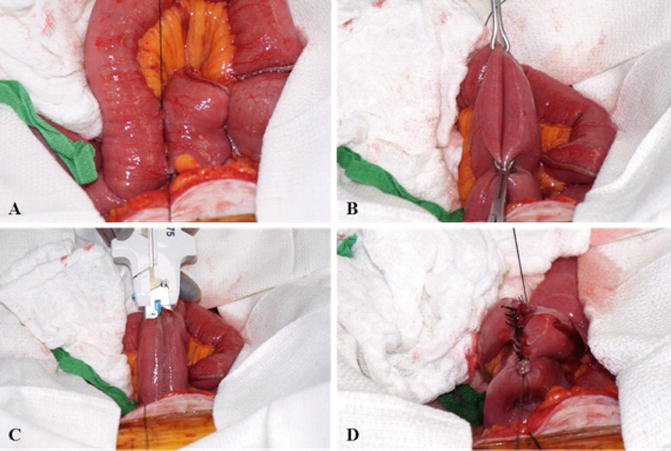




Fig. 13.3
Stapled anastomosis technique. (a) The divided ends are aligned in an isoperistaltic manner. (b) Full-thickness enterotomies are made on the antimesenteric bowel wall. (c) Side-to-side enteroenterostomy is made with the linear GIA stapling device. (d) The remaining defect is then closed with interrupted seromuscular sutures
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
