Fig. 1
Ileal obstruction due to stromal tumor. a Abdominal radiograph in supine position shows multiple dilated jejunal loops filled with gas. Dilated ileal loops are not visible because they are filled with fluid. These fluid-filled bowel loops are good acoustic window through which the dilated bowel loops and the cause of obstruction can be visualized. b Sonogram of the jejunum shows dilatation with markedly increased peristalsis, the fluid and tiny gas bubbles moving actively in the dilated bowel lumen. Note thick and compact valvulae conniventes. c Sonogram of the ileum shows dilatation with increased peristalsis. Note virtually absent valvulae conniventes (arrows). d Sonogram of the lower abdomen discloses a lobulated tumor (short arrows) arising from the ileum. Note dilated ileal loops (long arrows)
The use of sonography in the era of multidetector CT scanning is controversial. CT diagnosis of intestinal obstruction has decided advantage in terms of accuracy in diagnosis of bowel obstruction and in demonstration of the cause. Furthermore, interpretation of multidetector CT images is not so operator dependant as sonography. However, sonography is much more widely available than multidetector CT scanner, much cheap, and there is no radiation hazard. Therefore, sonographic examination may be tried in patients with normal plain radiographs or gasless abdomen, suspected obstruction in proximal bowel loops, in children, or in pregnant women (Ko et al. 1993b).
2 Pathology of Bowel Obstruction
Bowel obstruction is characterized by dilatation of the intestinal segments proximal to the site of obstruction and collapse of the segment distal to the obstruction. The dilated bowel contains a large amount of fluid, food stuff, or gas. There is increased peristalsis to attempt to pass the luminal content beyond the obstruction site. Bowel obstruction can be due to obturation by blockage of the lumen by bowel content, such as food stuff, bezoar, or gallstone, due to bowel wall abnormality, such as neoplasm or stenosis, and due to extrinsic causes, such as adhesion and hernia. In paralytic ileus, bowel is dilated and filled with fluid and gas, but there is no peristaltic movement.
3 Small Bowel Obstruction
Characteristic sonographic findings of small bowel obstruction are demonstration of dilated bowel loops with active peristalsis (Ko et al. 1993a). Multiple segments of dilated bowel loops can be readily demonstrated when the lumen is filled with fluid. The fluid may be clear or there may be air bubbles or debris. The dilated loops are continuous, the diameter of bowel lumen being over 2.0 cm and the segments being longer than 10 cm. Valvulae conniventes or intestinal folds are prominent and compact along the jejunum and thin and sparse along the ileum (Fig. 1). Sometimes, there is no valvular conniventes in the distal ileum and the bowel wall is flat. Increased peristalsis of the proximal segment of the bowel can be directly observed. The dilated bowel loop changes in caliber as well as in position, very vigorously, sometimes with some pauses. The fluid and tiny gas bubbles in the involved bowel show to-and-fro or whirling motion (Fig. 2). When the lumen is filled with gas, bowel dilatation is not easily recognized and it is difficult to make a diagnosis of bowel obstruction with sonography (Fig. 3). Usually, bowel contains both fluid and gas. Sonographer should try to avoid gas filled lumen by pressing the abdomen with transducer or change the position of the patient.
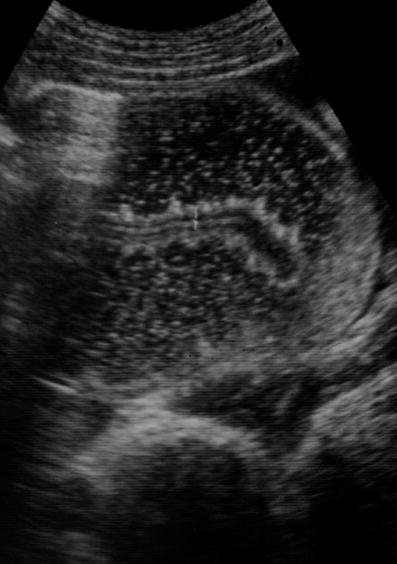
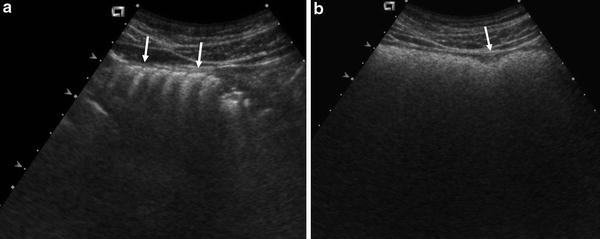
Fig. 2
Increased peristalsis. Sonogram of the jejunum shows dilated loop with increased peristalsis. The dilated loop shows vigorous change in caliber and in position. Tiny gas bubbles in the lumen show to-and-fro and whirling motion
Fig. 3
Gas filled distended bowel loops. a Sonogram of the gas filled jejunum shows air-trapping in the valvulae conniventes (arrows). b Sagittal sonogram along the right side abdomen shows gas filled, distended ascending colon. Note a haustral indentation (arrow)
The causes of bowel obstruction can be demonstrated (Ko et al. 1993a). Small bowel bezoar is usually caused by persimmons and orange, sometimes by cabbage, sauerkraut, potato peel or grapefruit. Patients who had subtotal gastrectomy or gastrojejunostomy are prone to develop bezoars.
Sonographically, bezoars are seen as an intraluminal mass with hyperechoic arclike surface casting clear posterior acoustic shadow (Fig. 4) (Ko et al. 1993b; Tennenhouse and Wilson 1990). Phytobezoar or trichbezoar are same in sonographic appearances. The obstructed small bowel loops usually contain a large amount of air and bezoars can be overlooked if sonographic examination is not done meticulously. Sonographic findings of gallstone ileus are identical to those of bezoars (Fig. 5) (Ko et al. 1993a, b; Davir 1991). Air in the biliary tree or nonvisualization of the gallbladder lumen may be a clue for gallstone ileus.
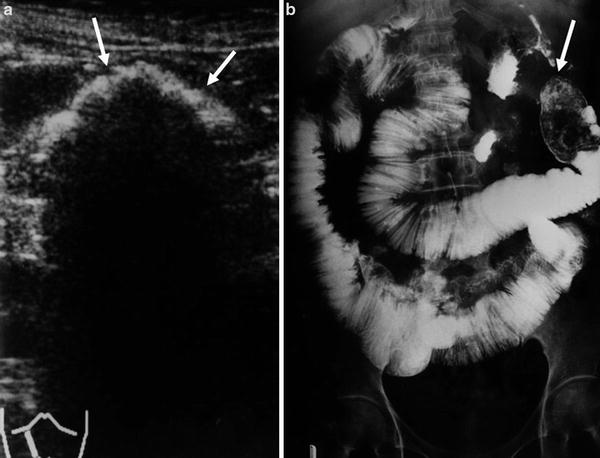
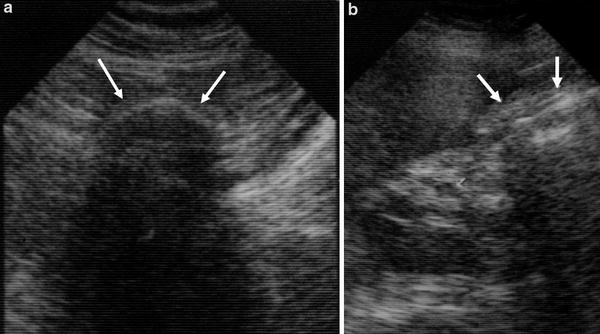
Fig. 4
Phytobezoar in the jejunum. a Sonogram of upper abdomen shows hyperechoic, arclike echo with clear acoustic shadow within a loop of the jejunum (arrows). Bowel loops proximal to the bezoar is dilated and filled with fluid. b. Small bowel follow-through examination shows a large intraluminal filling defect at the end of the dilated jejunum, representing bezoar (arrow)
Fig. 5
Gallstone ileus. a Sonogram shows hyperechoic arclike echo with posterior acoustic shadow within a dilated loop of ileum, representing a large gallstone (arrows). b Sonogram of the right upper abdomen discloses the gallbladder which is empty (arrows)
Small bowel tumor, either primary or metastatic, can be identified as a cause of bowel obstruction (Ko et al. 1993a). At the end of dilated small bowel or between the dilated bowel loops, a tumor can be identified when the tumor is sizable (Fig. 1). Fluid within the bowel may comes in direct contact with the mass indicating the mass arises from the bowel. There may be vascular structure in the mass visualized by applying Doppler study. Small bowel intussusception can be diagnosed by demonstration of bowel-within-bowel by recognizing characteristic multiple concentric rings, caused by invaginating layers of telescoped bowel, seen in cross section of the bowel loop.
Intestinal adhesion, the most frequent cause of bowel obstruction, cannot be demonstrated on sonography. Similarly, internal hernia and congenital fibrotic band can be rarely identified on sonography. Previous history of abdominal operation in patients without sonographically visible cause of obstruction can lead to a diagnosis of adhesive ileus.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


