, Min P. Kim2 and Shanda H. Blackmon1
(1)
Division of General Thoracic Surgery, Mayo Clinic, 200 First Street SW, Rochester, MN 55905, USA
(2)
Division of Thoracic Surgery, Department of Surgery, Houston Methodist Hospital, Houston, TX, USA
Keywords
Cervical esophageal perforationThoracic esophageal perforationAbdominal esophageal perforationEsophageal leakEsophageal fistulaEsophageal stentEsophagostomyEsophageal diversionEsophageal exclusionVenting gastrostomyFeeding jejunostomyEsophageal Perforations
Diagnosis of esophageal perforation can be made with a water-soluble esophagram followed by thin barium if no leak is seen with the water-soluble contrast. If there is still a concern for perforation after an esophagram, a CT scan is performed to evaluate for extraluminal air and extraluminal collection. The esophagus is divided into three parts: cervical, thoracic, and abdominal (Fig. 8.1). We recommend different management options based on the location of the perforation.
Fig. 8.1
The most common sites of cervical, thoracic, and abdominal esophageal perforations
Cervical Esophageal Perforation
Often, cervical esophageal perforation is treated by neck incision and washout of the wound. Nutrition and sepsis must be addressed. The patient is kept NPO with a Dobhoff feeding tube, a feeding tube placed surgically or by percutaneous endoscopy, or total parental nutrition (TPN). This combination provides the best opportunity to heal the leak. Esophageal stenting in this location is very difficult for the patient to tolerate. It leads to opening of the upper esophageal sphincter and higher risk of aspiration, so we typically rely on surgical drainage and antibiotics as treatment for cervical esophageal perforation.
Position
The patient is supine with a shoulder roll and the head turned towards the right side.
Operation
1.
Make an incision anterior to the left sternoclavicular muscle.
2.
Divide the omohyoid to expose the esophagus.
3.
Irrigate the left neck and leave a Jackson-Pratt (JP) or Penrose drain.
4.
Perform dressing changes.
Patient with Pneumomediastinum but Without Obvious Esophageal Leak
A patient with pneumomediastinum without any extravasation of contrast on esophagram or CT of the chest (Fig. 8.2) may be treated with NPO and IV antibiotics. Imaging should be repeated in at intervals to confirm the resolution of the pneumomediastinum and the lack of extraluminal fluid or contrast. Once the pneumomediastinum is resolved, the patient’s diet should be advanced. As a follow-up, the cause of the pneumomediastinum should be investigated, most commonly with esophagogastroduodenoscopy (EGD) initially.
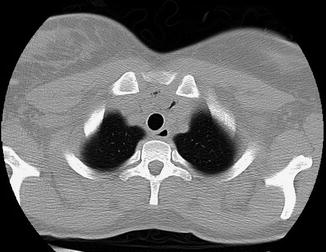
Fig. 8.2
CT scan demonstrating pneumomediastinum
Thoracic Esophageal Perforation
Patients without systemic sepsis and with evidence of thoracic esophageal perforation (Fig. 8.3) initially can be managed with esophageal stent placement, NPO, and IV antibiotics. Some smaller perforations or leaks without sepsis can be treated with endoluminal clips e.g. through the scope clips or over the scope clips (Fig. 8.4). Based on the degree of contamination of the mediastinum and the pleural space, the patient may require concomitant washout of the chest cavity. If the stent fails or if the leak from the perforation is large and the patient is systemically unwell, we perform surgical repair with intercostal muscle flap and wide drainage.

Fig. 8.3
Contrast swallow demonstrating a thoracic esophageal perforation
Fig. 8.4
Endoscopic treatment of an esophageal perforation using an over the scope clip. (a) Endoscopic appearances of esophageal perforation. * denotes the perforation. (b) Contrast esophagram demonstrating the esophageal perforation. (c) Combined endoscopic and radiological examination demonstrating the esophageal perforation and determining the correct positioning of the endoscope for clip deployment. (d) Deployment of the over the scope Ovesco clip to seal the esophageal perforation. (e) Endoscopic appearances of the esophageal perforation sealed by the Ovesco clip. (f) Contrast esophagram to demonstrate complete closure of the esophageal perforation by the Ovesco clip
Esophageal Stent
Position
The patient is supine.
Operation
1.
Perform endoscopy to determine the location of the perforation (Fig. 8.5).
Fig. 8.5
Endoscopic appearance of a large intra-thoracic anastomotic leak post-esophagectomy. The gastric conduit can be seen to the left and cavity formed from the anastomotic leak to the right of the image
2.
Irrigate the area with saline flushing from the endoscope.
3.
Mark the proximal and distal point of perforation using a paper clip taped on the skin of patient, using fluoroscopy
4.
Place a stiff guidewire into the stomach and remove the endoscope. Use fluoroscopy to ensure that the guidewire remains in the stomach.
5.
Place the delivery system over the wire into the area of the perforation. Place two thirds of the stent above the area of the perforation.
6.
Remove the delivery system.
7.
Perform an on-the-table esophagram to assess for a seal; then perform an awake swallow test.
8.
Place a bridle around the proximal point of the stent (Fig. 8.6), or alternatively use an Apollo OverStitch™ device (Apollo Endosurgery, Austin, TX) to suture the stent in place.
Fig. 8.6
Bridling the stent. One method for reducing the rate of stent migration is to “bridle” the stent. This involves hooking an umbilical tape through the proximal portion of the stent before placement. Once the stent is in place, the umbilical tape is carefully withdrawn through the esophagus and tied outside the nose to secure it. The stent depicted is a WallFlex™ stent (Boston Scientific, Marlborough, MA)
Thoracoscopic Washout of the Chest
Position
The patient is in a lateral decubitus position.
Operation
1.
Place the ports:
Initial working port: 1-cm incision 1–2 cm below the scapular tip, which allows the visualization of the two anterior ports
Camera port: 1-cm incision above the diaphragm in the posterior axillary line
Working port: 1-cm incision in the sixth intercostal space, in the anterior axillary line
2.
Perform washout:
Remove the contents of the perforation.
Irrigate the chest cavity with saline.
Decorticate the lung.
Place a chest tube in the area of the perforation.
Surgical Repair
If the leak is not sealed by the esophageal stent (Fig. 8.7), or if the perforation is large, primary closure with an intercostal muscle flap may be required. The lack of seal after stent placement is likely to be due to leakage from a proximal or distal point. Rarely, a hole in the middle of the stent may lead to a persistent leak. For a classification system of stent leakage and management, see Figs. 8.8 and 8.9. Exchange of the esophageal stent may seal the leak. If stent exchange or manipulation does not seal the leak, surgery is advised. For the best opportunity to seal the leak, we advise leaving the esophageal stent in place while performing the closure and muscle flap (Fig. 8.10).