Fig. 15.1
CT shows the liver mass in the central lobe, which is operated by partial resection. On the edge of the tumor, the traction lines are sutured. It is beneficial for exposure and dissection and easy to operate
15.8.9 Surgical Margins
Generally, the more generous the tumor margin is, the more thorough the surgery is. Margins in a particular patient depend on the tumor location and size and the degree of the liver cirrhosis. The rate of radical surgery increases with the use of extended surgical margins; however, safety is relatively decreased, as important vascular branches can be damaged due to blind expansion of the scope of the resection. Traditionally, surgical margins should be >1 or 2 cm; however, these boundaries have not been confirmed in current studies [8]. Some professors believe that satisfactory margins can be achieved with R0 resection [9]. Indeed, the use of intraoperative ultrasound is needed to define the tumor margins to avoid the mistakes of missing or cutting through the tumor.
15.8.10 Methods and Skills for Liver Transection
There are multiple ways to transect the liver: the simple forceps method (using a rectangular clamp hook with ligation and the Kelly clamp crushing method), ultrasonic crushing of the liver parenchyma (using CUSA, water jet, ultrasonic aspirator, etc.), the energy pliers clamp method (BiCamp, LigaSure, etc.), the energy curing transection method (microwave coagulator, Habib 4×, radio frequency, etc.), and a combination of these methods. Actually, there is no difference in complications among these different methods, and surgeons should use the method in which they are most skilled [10]. We recommend the liver parenchyma ultrasonic crushing method, which transects tissue quickly and ensures a handling of the transected bile ducts and vessels, therefore reducing postoperative tissue necrosis and inflammation, especially in complex and larger cross-sectional liver resections. Moreover, this method is the basic technique for precious liver resection and living-donor liver resection [11] (Fig. 15.2).
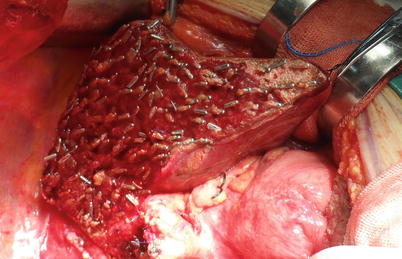
Fig. 15.2
The transected section by right hemihepatectomy with water-jet method
15.8.11 Surgical Strategies
In HCC, intrahepatic metastasis usually occurs via the portal vein. Based on this principle, anatomical liver lobe or segment resections are performed, although it remains unknown whether anatomical liver resection is more radical (Fig. 15.3). Because 80 % of HCC patients also have liver cirrhosis, liver resection often follows the rule of “anatomical left hepatectomy, nonanatomical right.” That is to say, left lobectomy or hepatectomy is recommended for left-sided tumors; for right-sided tumors, a right partial hepatectomy is performed. A detailed list of recommendations for resection follows. ① For tumors in segments II and III, an anatomical left lateral lobe resection is performed. ② When the tumor is located at the border of the left lateral and medial lobes, or in cases of deeper tumors or tumors that are larger than 5 cm, an anatomical left hepatectomy is performed. ③ When the tumor is in segments IVa and IVb and is less than 3 cm in size, a partial IVa or IVb segmentectomy is performed. ④ When the tumor is located in the left medial lobe and is larger than 3 cm in size, a IV segmentectomy is performed. ⑤ For tumors that are larger than 5 cm and involve the right lobe, a right hepatectomy is performed. ⑥ In superficial tumors that are smaller than 3 cm, a partial liver resection is performed. ⑦ When the tumor is limited to segments V, VI, VII, and VII and is smaller than 3 cm, a segmentectomy is performed. ⑧ When the tumor involves adjacent segments, a combined liver resection is performed. ⑨ For tumors limited to the caudate lobe, the whole caudate lobe should be resected. ⑩ If a caudate lobe tumor invades the left or right lobe of the liver, a combined liver resection is performed.
Fig. 15.3
 Liver Anatomy and the History of Hepatectomy
Long-Term Outcomes of Liver Resection
Liver Anatomy and the History of Hepatectomy
Long-Term Outcomes of Liver Resection
 Native Liver Resection in Liver Transplantation
Native Liver Resection in Liver Transplantation
 Associating Liver Partition and Portal Vein Ligation for Staged Hepatectomy
Associating Liver Partition and Portal Vein Ligation for Staged Hepatectomy
 Procurement of Liver Graft
Procurement of Liver Graft
 Surgical Treatment of Hepatocellular Carcinoma Accompanied with Portal Vein Tumor Thrombus
Surgical Treatment of Hepatocellular Carcinoma Accompanied with Portal Vein Tumor Thrombus




CT shows the liver mass is in the segment IV. The patient could tolerate left hemihepatectomy with a physical and liver condition. The Postoperative pathological report shows moderate differentiated hepatocellular carcinoma with microvascular invasion
Related posts:
Liver Anatomy and the History of Hepatectomy
Long-Term Outcomes of Liver Resection
Native Liver Resection in Liver Transplantation
Associating Liver Partition and Portal Vein Ligation for Staged Hepatectomy
Procurement of Liver Graft
Surgical Treatment of Hepatocellular Carcinoma Accompanied with Portal Vein Tumor Thrombus
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
