Fig. 31.1
The midline incision on the chest and abdominal wall
3.
Resect the pericardium and perform heart decompression. This procedure can promote the blood of the abdominal organs to flow into the heart and reduce organ congestion and edema. Keep the diaphragm intact (Fig. 31.2). Cut off the falciform ligament to the second hepatic portal.
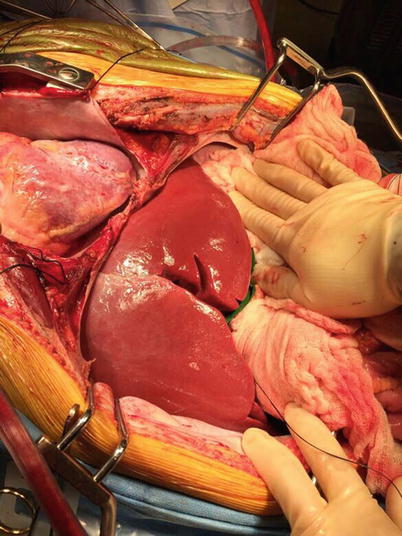
Fig. 31.2
Revealed heart, lungs, and liver
4.
Check the condition of the liver: whether the color is normal, the texture is soft, the edge is sharp, and whether the presence of nodule. Fig. 31.2). If the liver is swelling, a dose of 50-100 g of 20 % Mannitol should be intravenously infused; if blood pressure is stable, a dose of 20-100mg of Lasix should be intravenously infused at the same time.
5.
Carefully check the branches at the first hepatic portal. Any variations of the right hepatic artery [usually originating from the superior mesenteric artery (SMA)] should be protected. If the variant artery is located behind the pancreas, the pancreas graft can be used. If the variant hepatic artery transverses the pancreas, do not use the pancreas graft and protect the liver graft.
6.
Free and remove the left hepatic ligament; then, ligate the gastrohepatic ligament. The upper edge of pancreas is seen near the lesser curvature of the stomach. If there is any variant left hepatic artery (usually from the left gastric artery), it needs protection. Ligate the gastrocolic ligament. The entire pancreas is revealed behind the stomach. Check whether the pancreas is pink, soft, smooth, and without nodules. Check whether the pancreatic head is big and the pancreatic body and tail is thin and short. Cover the pancreas with wet gauze to avoid mechanical extrusion.
7.
Open the pelvic peritoneum on the upper edge of the pelvic, expose the end part of the abdominal aorta and place 0-silk suture for traction. (Fig. 31.3).
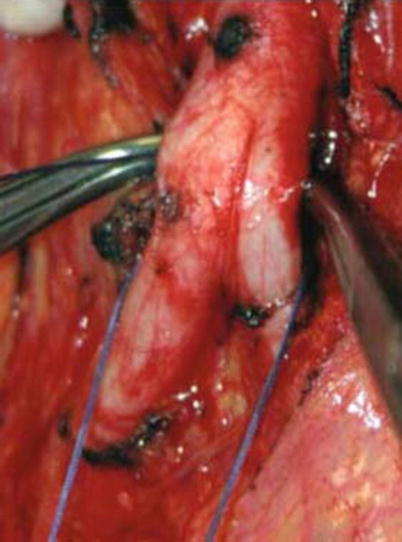
Fig. 31.3
The inferior segment of the abdominal aorta
8.
Reveal the inferior mesenteric vein (IMV) at the left abdomen and place traction sutures to retract it (Fig. 31.4). Along the retroperitoneum, find and isolated the initial portion of the SMA and set into the traction. Do not ligate the peripheral vasculature of the SMA to avoid affecting the blood supply and venous drainage of the pancreas.
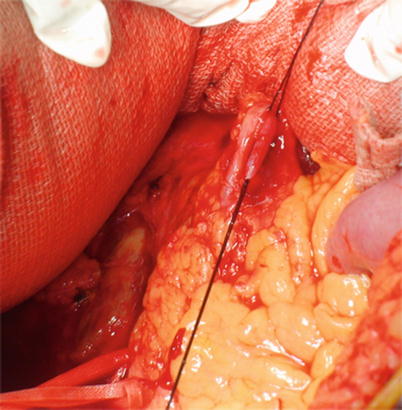
Fig. 31.4
The inferior mesenteric vein
9.
Dissect the trunk of the celiac artery on the upper edge of the pancreas. Isolate the splenic artery and place traction sutures on the initial section (Fig. 31.5). Isolate the gastroduodenal artery (GDA) at the end of the common hepatic artery and place traction sutures behind the initial section of GDA (Fig. 31.6).
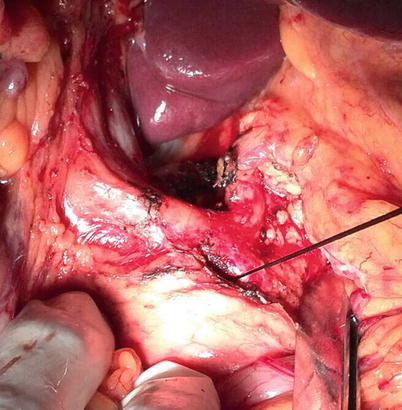
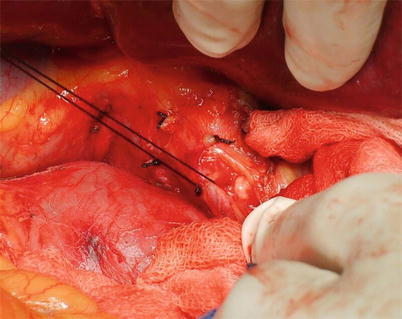
Fig. 31.5
The origin of the splenic artery
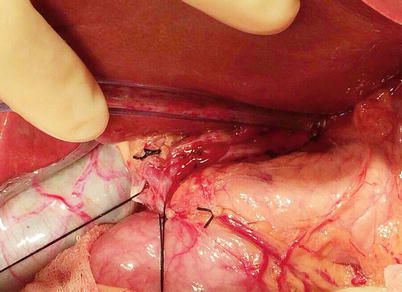
Fig. 31.6
Separation of the GDA and placement of the traction sutures
10.
Isolate and cut off the common bile duct near the pancreatic head (Fig. 31.7).