Fig. 26.1
(a, b) Portal vein embolization to induce FLR regeneration
Two-stage hepatectomy proposed by Adam, 2000: First, resect the tumors from the FLR (infrequently, this step is combined with PVE); then, perform the hemihepatectomy after the FLR regenerates (Fig. 26.2) [2].
Fig. 26.2
(a, b) Tumor resection of the FLR combined with PVE to induce FLR regeneration
Two-stage hepatectomy proposed by Clavien, 2007: Perform a wedge-shaped resection of all left-side tumors, and ligate the right portal vein during the first stage. Complete the extended right hemihepatectomy when the left lobe is adequately regenerated, after a few weeks (Fig. 26.3) [4].
Fig. 26.3
(a, b) Tumor resection of the FLR and ligate the right portal vein to induce FLR regeneration
Characteristics of the two-stage hepatectomy:
Advantages:
This procedure stimulates FLR regeneration and leaves open operative opportunities for patients with giant liver cancer [6].
Limitations:
(1) The tumor may progress in the long interval between the two stages, which exceeds an average of 4 weeks. (2) The adhesion that results from the first stage may make the second stage more difficult. (3)FLR regeneration may not be satisfactory (10–46 % in 2–8 weeks) [7].
26.4 Initial Proposition of ALPPS
Schnitzbauer summarized the clinical data of 25 cases of ALPPS in five centers in Germany, constituting the initially proposed technique (Fig. 26.4).
Fig. 26.4
(a, b) The right portal vein is ligated with in situ splitting to induce rapid remnant liver regeneration
Advantages:
(1) The adhesion can be easily handled due to the short interval (~1 week) between the two surgeries. (2) The FLR regenerates rapidly, within 7 days after the first surgery (74–87 %). (3) The tumors in the FLR or in other organs can simultaneously be resected in the first stage [7].
Limitations:
(1) High morbidity (53–90 %) and mortality (0–28 %) and (2) no report on long-term outcome.
26.5 Indication
(1) Normal liver, FLR <30 %; (2) liver with jaundice or cirrhosis, FLR <40 %; (3) liver metastases from colorectal cancer, giant HCC, or ICC; or (4) FLR cannot reach the expected volume after PVE
26.6 Contraindication
26.7 Technical Points
1.
2.
Operation method: Open or laparoscopic
Technical Points of Open ALPPS
1.
Choice of incision
An inverted “L” incision is regularly adopted due to the better operative field and convenient hilar handling (Fig. 26.5).
Fig. 26.5
The inverted “L” incision in the right upper abdomen
2.
Skeletonize the first portal and expose the hepatic artery, bile duct, and portal vein. Then, ligate the portal vein if needed. Wrap silk sutures around the hepatic artery and bile duct to ligate during the second stage (Fig. 26.6).
Fig. 26.6
(a) Skeletonize and ligate the portal vein; (b) wrap silk sutures around the hepatic artery
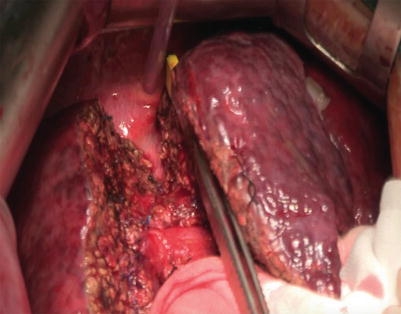
3.
Parenchymal dissection with an anterior approach to the caval vein. Maintain rigorous hemostasis on bilateral sections and ligate the bile capillary (Fig. 26.7).