Embryology and Histology of the Uterus
Michael S. Baggish
Leslie B. Arey
Embryology
The Bisexual Primordia
The human embryo of 8 weeks is provided with two pairs of potential genital ducts. The male pair originates as the mesonephric ducts of the provisional midkidneys; however, because at this stage gonadal sex is becoming established, these ducts soon regress, leaving remnants near the ovaries and the so-called Gartner ducts in regions between the ovaries and hymen. The female ducts, by contrast, are created specifically for genital purposes.
The first indication of each female duct is a groove on the lateral surface of each mesonephros that appears in embryos of nearly 6 weeks’ development (Fig. 1.1). This groove indents the superficial epithelium, and its lips promptly close, thereby creating a detached tube that advances caudally within the mesonephric ridge. This female duct was originally named the müllerian duct but is now known officially as the paramesonephric duct (Fig. 1.2). Near the cloaca of the embryo the two ridges bearing the ducts swing toward the midplane and fuse into a cylindrical mass called the genital cord (Fig. 1.3). At this time (7 weeks), the two internal tubes are still separate but have nearly reached the cloaca.
Uterine Morphogenesis
In embryos of 10 weeks, the general plan of the female duct system is evident (Fig. 1.4). The cranial segments of both ducts persist as uterine tubes. Slanting middle segments of both ducts will soon merge and give rise to the fundus of the uterus. The caudal segments of the ducts, already fused, become the corpus cervix and much of the vagina. The caudal end of the now single tube presses against the urogenital subdivision of the cloaca, the joint membrane then representing the future hymen. The early uterus lacks a fundus as such, and hence is bicornuate (Figs. 1.4 and 1.5A). After a time the cranial walls of the slanting segments bulge in a
cranial direction, so that their original angular junction (Fig. 1.5A) becomes flat (Fig. 1.5B) and finally a dome (Figs. 1.5C and 1.6).
cranial direction, so that their original angular junction (Fig. 1.5A) becomes flat (Fig. 1.5B) and finally a dome (Figs. 1.5C and 1.6).
 FIGURE 1.1 Urogenital ridge of the human embryo: 9-mm ventral view. (From Arey LB. Developmental Anatomy. 7th ed. Philadelphia: WB Saunders; 1974, with permission. ) |
 FIGURE 1.2 Origin of the müllerian ducts, illustrated by transverse sections through the early urogenital ridge. A: Infolding of the peritoneum (mesothelial lining). B: Narrowing of the neck of the invaginated mesothelium. C: The neck is pinched off, and a free tube is formed. (From Arey LB. Developmental Anatomy. 7th ed. Philadelphia: WB Saunders; 1974, with permission. ) |
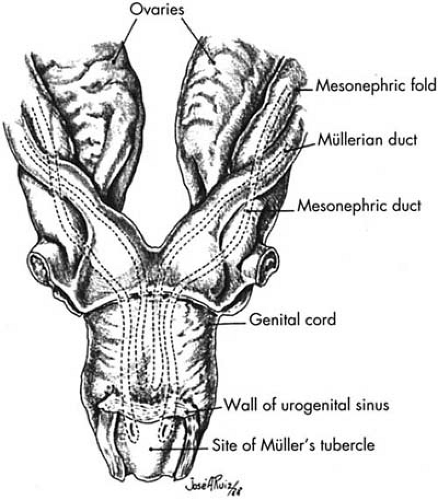 FIGURE 1.3 Course of the müllerian ducts and formation of the genital cord at 2 months. (From Arey LB. Developmental Anatomy. 7th ed. Philadelphia: WB Saunders; 1974, with permission. ) |
 FIGURE 1.4 Female genital tract at 10 weeks. (From Arey LB. Developmental Anatomy. 7th ed. Philadelphia: WB Saunders; 1974, with permission.) |
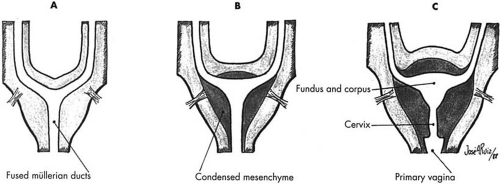 FIGURE 1.5 Diagrams of the later progress of the transverse limbs and fused müllerian ducts. (From Arey LB. Developmental Anatomy. 7th ed. Philadelphia: WB Saunders; 1974, with permission. ) |
 FIGURE 1.6 Female genital tract at birth. (From Arey LB. Developmental Anatomy. 7th ed. Philadelphia: WB Saunders; 1974, with permission. ) |
The uterine epithelium buds off glands by the seventh prenatal month, and this establishes the endometrium; yet, they remain small until the child reaches puberty. A distinction between uterus and vagina becomes evident at the middle of the fourth month when the fornices appear. The muscular wall, or myometrium, of the uterus is indicated at 3 months by mesenchyme of the genital cord condensing into smooth muscle fibers that invest the endometrium. The parametrium differentiates from the exterior of the genital cord into a peritoneal covering (mesothelium and connective tissue). The uterus grows rapidly in the final months of
fetal development, and the cervix becomes the longest segment by far. Shortly after the child’s birth, the uterus loses one half of its length, mostly at the expense of the cervix. It does not recoup this loss until the onset of puberty. The state of the female genitals at birth is shown in Figure 1.6.
fetal development, and the cervix becomes the longest segment by far. Shortly after the child’s birth, the uterus loses one half of its length, mostly at the expense of the cervix. It does not recoup this loss until the onset of puberty. The state of the female genitals at birth is shown in Figure 1.6.
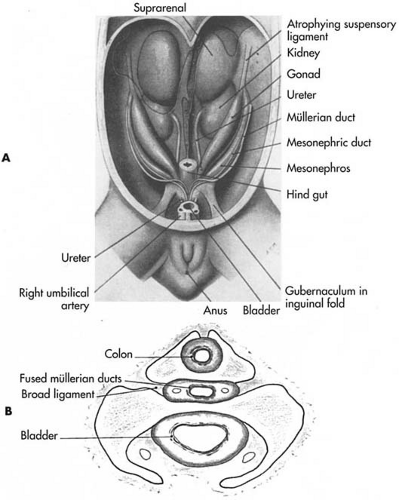 FIGURE 1.7 A: Schema of the excretory organs and reproductive structures at 6 to 8 weeks of life. B: Transverse section through the lower trunk at approximately 3 months. (A: From Jones HW Jr, Scott WW. Hermaphroditism, Genital Anomalies, and Related Endocrine Disorders. 2nd ed. Baltimore: Williams & Wilkins; 1971, with permission. B: From Arey LB. Developmental Anatomy. 7th ed. Philadelphia: WB Saunders; 1974, with permission. ) |
The Uterine Ligaments
The uterine ligaments are logical survivors in relation to the development of the uterus itself. The two genital ridges, containing the paired müllerian ducts, swing together and meet, thereby providing a horizontal shelf that bridges between the right and left body walls (Fig. 1.7). It contains the uterus in its midportion. The shelf itself persists as the sheetlike broad ligaments, fibromembranous in composition (Fig. 1.7). Portions of the genital ridges unite the caudal end of each ovary to the slanting segments of the genital ridges that become the cranial end of the uterus. The sites of uterine attachment are lateral. These bands become fibromuscular and are known as the proper ligaments of the ovaries (Figs. 1.7 and 1.8). By the beginning of the third fetal month, continuous cords extend from the upper lateral regions of the uterus into the swellings that become the labia majora. They represent the linkage of two strands: the inguinal ligaments to the body wall at the sites of the future inguinal canals, and the labial ligaments extending into the labia majora. The total lengths of the compound cords become fibromuscular and are named the round ligaments (Fig. 1.8). The cardinal ligament develops as a fibrous sheet of fascia embedded in the lateral wall of the cervix; it is a deeper continuation of
the broad ligament. The uterosacral ligament differentiates from mesenchyme as a fascial band extending from the cranial part of the cervix to the sacrum.
the broad ligament. The uterosacral ligament differentiates from mesenchyme as a fascial band extending from the cranial part of the cervix to the sacrum.
 FIGURE 1.8 The genital ligaments at 10 weeks. R, round ligament of the uterus; S, suspensory ligament of the ovary; PL, proper ligament of the ovary. (From Arey LB. Developmental Anatomy. 7th ed. Philadelphia: WB Saunders; 1974, with permission. ) |
Uterine Anomalies
The most common departure of the uterus from its normal configuration results from failures of the müllerian ducts to unite completely or to form a fundus. Figure 1.9 illustrates the conditions affecting both the uterus and the vagina; Figure 1.9 shows a double uterus alone; Figure 1.9 illustrates a largely bipartite uterus with a variably persistent median septum; and Figure 1.9 shows a bicornuate uterus in which the domed fundus fails to form. All of these differences are incorporated in the final adult states of various subprimate mammals. Retention of the infantile size of the uterus results from an inadequate supply of pubertal estrogen or a failure of normal tissue response. Congenital absence of the total uterus is rare.
Experimental Embryology
As described by Yost, the testis differentiates several weeks before the ovary; therefore male organogenesis precedes female organogenesis. Figure 1.10 shows schematically sexual differentiation of the sex ducts in rabbit fetuses. Note, if the animal is castrated in utero, differentiation of the ducts will proceed in the female direction (i.e., the müllerian ducts will form tubes, uterus, and vagina, and the male ducts will suppress).
The testes may be considered the conductor of the sexual differentiation train of events. Two substances or controllers are liberated by the testes: a polypeptide, the müllerian inhibiting factor, and a steroid hormone, testosterone. The latter enhances growth of the mesonephric ducts and their derivatives. Experiments in rabbits show that partial masculinization in female rabbits can result by grafting a testis onto a female fetus and subsequently observing the action of that alteration. The müllerian duct on the side of the graft was inhibited (Fig. 1.11). To further illuminate the two separate actions of the fetal testes’ actions on the genital tract, a crystal of testosterone was implanted in a female (XX) rabbit fetus in place of a testis. The results of that experiment showed that the müllerian ducts’ development was not inhibited, but the male mesonephric ducts were stimulated to develop synchronously with them (Fig. 1.12).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


