Chapter 41 DISTAL URETHRAL POLYPROPYLENE SLING
The sling procedure, first described in 1907 by Von Giordano, has been used for the treatment of female stress urinary incontinence (SUI) for almost 100 years.1 This procedure was reintroduced in 1978 by McGuire and Lytton, who used autologous rectus fascia suspended under the bladder neck for the treatment of intrinsic sphincter deficiency.2 In the past 25 years, a significant number of surgical procedures have been devised for the treatment of SUI, including multiple sling variations. A meta-analysis of various surgical techniques used in the treatment of SUI revealed that slings have similar durability to retropubic suspensions and are more efficacious than transvaginal suspensions and anterior repairs.3 In the past decade, slings have gained popularity, because new surgical techniques, sling materials, and an-choring methods have led to decreased surgical morbidity and convalescence time while providing good durability and ease of placement.
MID-DISTAL TO DISTAL SUBURETHRAL SLINGS
Slings were classically reserved for the treatment of SUI in the absence of urethral hypermobility. Although the exact mechanism by which slings restore continence remains elusive, the introduction and success of the mid-distal to distal slings have expanded understanding of the urethral support and continence mechanism. Klutke and colleagues demonstrated that anatomic correction of bladder neck hypermobility was not necessary to cure SUI.4 The tension-free vaginal tape (TVT), introduced in 1996, has been shown to be an effective treatment for SUI.4–18 Studies have demonstrated the TVT procedure to be as effective as open colposuspension, with documented cure rates of 81% and an improvement rate of 94%.19 Given the success of the TVT and based on the same anatomic principle and mechanism of action, other procedures such as SPARC (American Medical Systems, USA), Safyre (Promedon, Argentina), SABRE (Mentor Corporation, USA), and the transobturator tape (TOT; Mentor), among others, have been described for the treatment of SUI. All of these procedures involve the placement of a synthetic sling at the level of the mid-distal to distal urethra and are available as commercially packaged kits that include placement needles or passers and prefabricated slings. The primary difference is the approach to placement (i.e., from the suprapubic area to the vagina or from the vagina to the suprapubic area), sling length, passage through the retropubic region or not, and variations in the hardware necessary for placement. The special equipment requirements along with the high cost of the packaged kits make it difficult to use these devices in many parts of the world. Additionally, many of these techniques are done blindly without finger guidance, which can lead to high rates of bladder perforation and rare but major complications such as bowel or major vessel injuries resulting in severe morbidity.20–22
DUPS uses the same anatomic location and therapeutic principles as the other mid-distal slings described mentioned earlier, and it has been shown to be effective in the treatment of SUI.23,24 However, it has a lower risk of major injuries, because the sling is placed under tactile guidance through the retropubic space. The sling used is a 10 × 1 cm, short piece of soft, loosely woven mesh with large pores attached to absorbable sutures. Although the sutures traverse the retropubic space, the mesh itself traverses only 2 to 3 cm on each side into the retropubic space, because the presence of a small segment of mesh in the retropubic space is an important factor to cure SUI. Most of the other slings are self-fixating to the abdominal wall or the obturator muscle; DUPS uses a short segment of mesh attached to absorbable sutures for temporary support of the mesh until it becomes incorporated. This avoids complications such as infection or inguinal pain secondary to nerve entrapment from the suprapubic fixation while providing adequate attachment and fixation to the retropubic space. Additionally, these mesh properties lessen the chance of complications such as mesh erosion into the urethra. DUPS is a simple, quick, and inexpensive procedure with a lower risk of major complications compared with other slings.
SURGICAL TECHNIQUE
The patient is placed in high dorsal lithotomy position. The lower abdomen and genitalia are prepared and draped in sterile fashion, the labia are retracted laterally with stay sutures, and the bladder is emptied with a 16-Fr urethral Foley catheter. A weighted vaginal speculum is used for exposure. An Allis clamp is used to grasp the anterior vaginal wall just proximal to the meatus. Two oblique lateral incisions are made in the anterior vaginal wall (Fig. 41-1). Another Allis clamp is placed at the distal end of each of the oblique incisions, and the dissection is carried out laterally over the glistening periurethral fascia toward the ipsilateral shoulder. The retropubic space is entered at the level of the mid-distal to distal urethra, using curved scissors directed parallel to the urethra just under the pubic bone (Fig. 41-2).
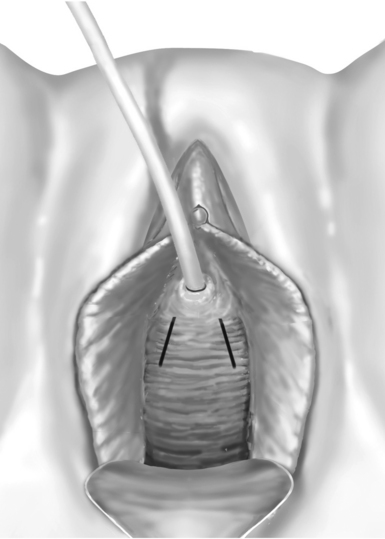
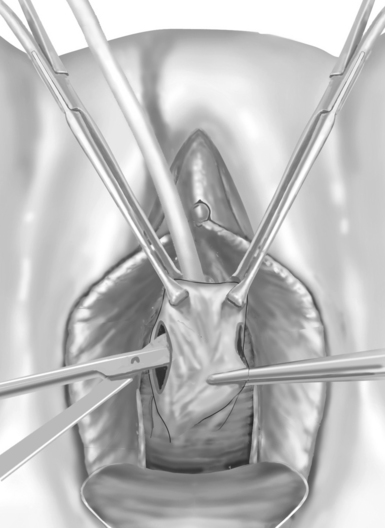
Figure 41-2 The retropubic space is entered at the level of the mid to distal urethra using curved scissors.
Related posts:
 DEVELOPMENTAL ANATOMY AND UROGENITAL ABNORMALITIES
DEVELOPMENTAL ANATOMY AND UROGENITAL ABNORMALITIES
 USE OF CADAVERIC FASCIA FOR PUBOVAGINAL SLINGS
USE OF CADAVERIC FASCIA FOR PUBOVAGINAL SLINGS
 EPIDEMIOLOGY OF INCONTINENCE AND VOIDING DYSFUNCTION IN THE ELDERLY
EPIDEMIOLOGY OF INCONTINENCE AND VOIDING DYSFUNCTION IN THE ELDERLY
 TRANSVAGINAL CLOSURE OF THE BLADDER NECK IN THE TREATMENT OF URINARY INCONTINENCE
TRANSVAGINAL CLOSURE OF THE BLADDER NECK IN THE TREATMENT OF URINARY INCONTINENCE
 FEMALE SEXUAL FUNCTION AND DYSFUNCTION
FEMALE SEXUAL FUNCTION AND DYSFUNCTION
 FUNCTIONAL ANATOMY AND PATHOPHYSIOLOGY OF PELVIC ORGAN PROLAPSE
FUNCTIONAL ANATOMY AND PATHOPHYSIOLOGY OF PELVIC ORGAN PROLAPSE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


