Fig. 1
Transverse scan of the gastric body. The 5-layer structure of the gastric wall and the gastric fold is demonstrated
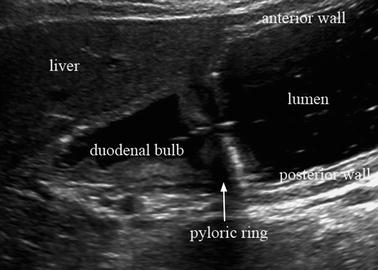
Fig. 2
Longitudinal scan of the gastric antrum, pylorus, and the duodenal bulb. Gastroduodenal lumen is filled with water
The normal gastric wall is demonstrated as a five-layer structure (Fig. 3). The first layer is hyperechoic, and corresponds to the luminal boundary and the part of the mucosal layer. The second layer is hypoechoic and includes the remaining part of the mucosa and mucosal muscle layer. The third layer is hyperechoic and corresponds to the submucosal layer. The fourth layer is hypoechoic and corresponds to the proper muscle layer. The fifth layer is hyperechoic and corresponds to the serosa and the extramural boundary.
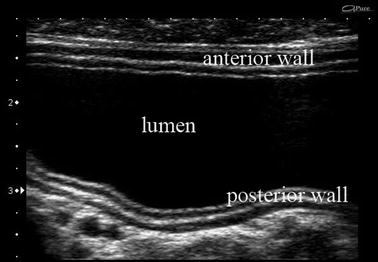
Fig. 3
The close-up view of gastric antrum. The 5-layer structure is clearly demonstrated
3 Sonographic Features of Gastric Cancer
3.1 Early Gastric Cancer
It is not always easy, and often rather difficult to detect early gastric cancer by means of usual ultrasonographic screening because both the wall thickening and alteration of wall stratification are too subtle to be detected with transabdominal ultrasound. In this respect, ingestion of water is useful to obtain a clear image of such subtle changes.
Early gastric cancer is usually expressed as focal wall thickening originating in the second layer. No changes of the submucosal layer are shown with intramucosal cancer (Fig. 4). When the tumor invades the submucosal layer, the shape and the width of that layer changes (Fig. 5) and it finally disappears as the tumor invades proper muscle.
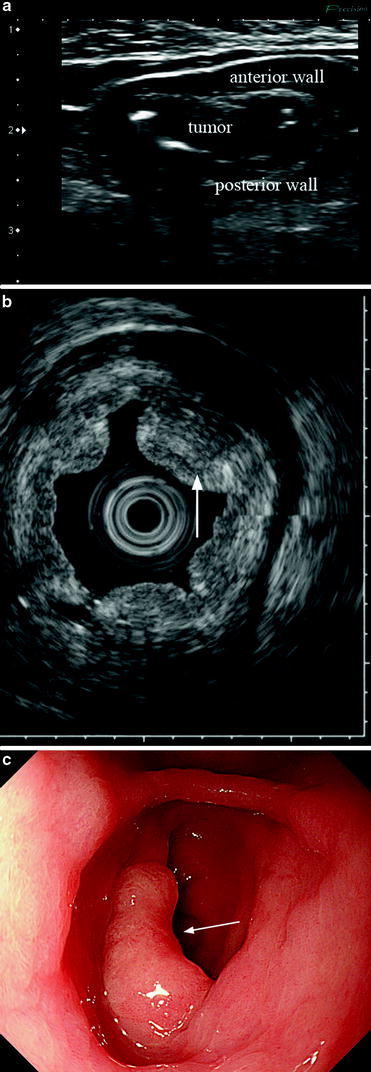
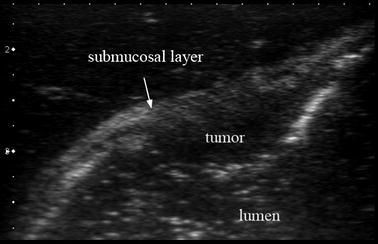
Fig. 4
Sonographic image of early (intramucosal) gastric cancer. a Focal wall thickening is demonstrated. The thickening is limited to the mucosal layer. b Echo-endoscopic feature of the same patient as shown in a. Focally elevated lesion is visualized (arrow). c Endoscopic image of the same. The lesion is recognized as the focal elevated area (arrow)
Fig. 5
Sonographic image of early (deep submucosa) gastric cancer. The blurring of submucosal layer indicates the deep submucosal invasion
However, the evaluation of cancer invasion becomes difficult when it is complicated by an ulcer because the fibrosis accompanying ulcer healing is expressed as a hypoechoic area which resembles cancer (Fig. 6).
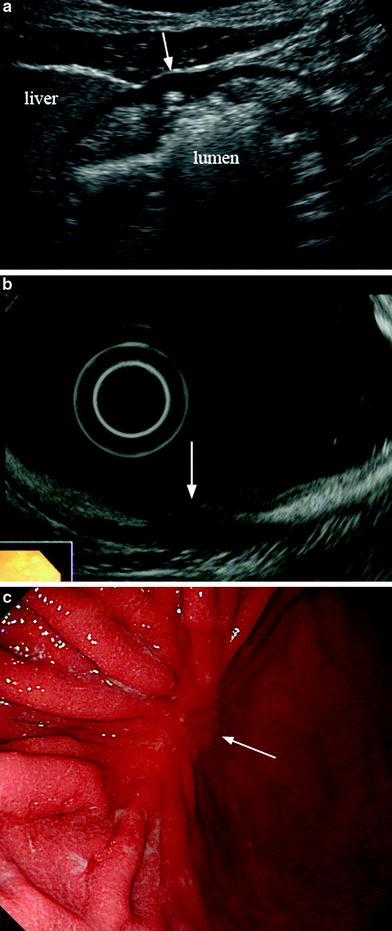
Fig. 6
Sonographic feature of advanced (mostly intramucosal with minute invasion into proper muscle) gastric cancer, complicated with ulcer scar (arrow). a Although the wall stratification has disappeared, the wall thickness is rather thinner than the normal gastric wall. b Endoscopic ultrasonography of the same lesion (arrow). c Endoscopic view of the same lesion. Ulcer scar is demonstrated (arrow)
The diagnostic accuracy of determination of cancer depth with transabdominal ultrasound is generally thought to be inferior to that with endoscopic ultrasound, which provides a clear image with fewer artifacts and high resolution, although there are several contradictive reports (Ishigami et al. 2004; Meining et al. 2002). Even with endoscopic ultrasound, however, it is difficult to differentiate fibrotic tissue from cancer.
3.2 Advanced Gastric Cancer
Advanced gastric cancer is demonstrated as focal wall thickening without wall stratification. The typical sonographic figure is a “pseudokidney sign”; i.e., an echogenic area surrounded by a hypoechoic rim that resembles the image of kidney (Fig. 7).

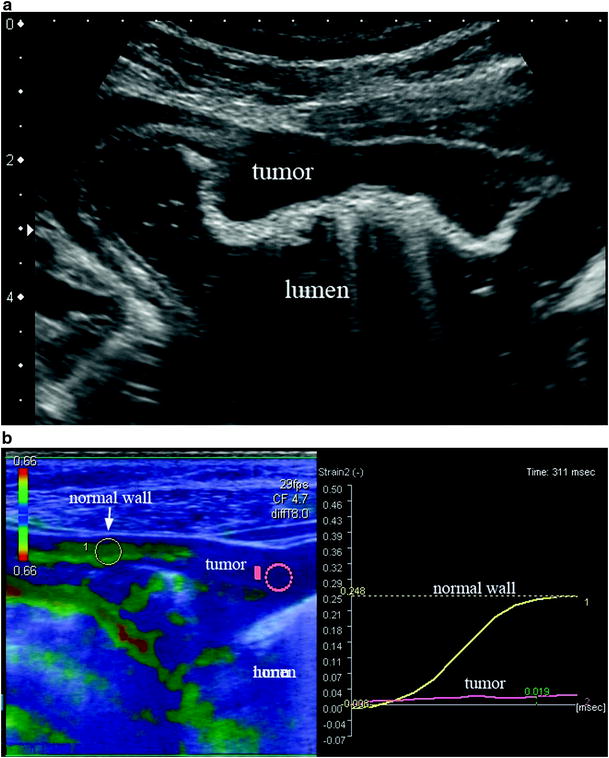
Fig. 7
Sonographic feature of an advanced gastric cancer showing the so-called “pseudokidney sign”
In most cases, although, the advanced cancer only shows eccentric or segmental wall thickening without wall stratification, which does not actually mimic the shape of kidney (Fig. 8a). In addition, sonographic evaluation of tissue elasticity has become possible recently to help us distinguish cancer from other disorders showing gastric wall thickening (Fig. 8b).