Anatomy of the Uterus
Michael S. Baggish
Gross Anatomy
The uterus occupies an anterior and central position in the pelvis. In its nonpregnant state, the uterus weighs between 30 and 80 gm. The uterus lies midway between the urinary bladder and the rectum.
The uterus is supported in the pelvis by the round, broad, uterosacral, and cardinal ligaments. The round and broad ligaments provide only a modicum of structural support, whereas the cardinal and uterosacral complex is strategic. These so-called ligaments are, in fact, not ligaments but rather condensations of the endopelvic fascia. The round ligament is composed of smooth muscle. The endopelvic fascia comprises areolar tissue, vascular structures, and nerves. True pelvic fascia refers to the sheaths covering the pelvic floor and sidewall striated musculature. The round ligament and ovarian vessels support a tentlike cover of peritoneum, the broad ligament. This is filled with fat and contains at its floor the uterine vessels, nerves, lymph vessels, and nodes. The blood supply to the uterus is plentiful and emanates from the anterior division of the internal iliac artery.
The uterus is a hollow, pyriform, muscular structure measuring 7 to 8 cm in length, 4 to 5 cm in width at its upper portion, and 2 to 3 cm in thickness. The uterus is divided into three portions: the cervix, corpus, and fundus. The narrowed area between the cervix and body is called the isthmus and corresponds to the level of the internal os or the opening between the cervical canal and the uterine cavity (Fig. 2.1).
The cervix is cylindrical and measures 3 to 4 cm in height and 2 cm in diameter. Its posterior extent is covered with peritoneum, which is reflected from the back of the vagina. The anterior portion of the supravaginal cervix is separated from the bladder by endopelvic fascia. Laterally the cervix is bounded by the structures lying within the broad ligament (Fig. 2.2).
The vaginal portion of the cervix projects into the vaginal canal and is surrounded by four vaginal fornices. It comprises approximately 70% of the cervical substance. The terminus of the cervix is rounded and is punctuated with a circular or transverse opening, the external os (Fig. 2.3). Two lips are identified, the anterior, which is shorter and thicker, and the posterior, which is longer and thinner. The portio vaginalis of the cervix usually enters the vagina obliquely from ventral to dorsal, pointing to the posterior wall of the vagina.
The canal of the cervix is for all practical purposes spindle shaped. Longitudinal crests of endocervical mucosa protrude into the cavity anteriorly and posteriorly as the plicae palmatae (Fig. 2.4A). Secondary oblique branching of the mucosa gives the appearance of a tree and constitutes the arbor vitae (Fig. 2.4B). The endocervical mucosa is whitish pink and, as noted, is thrown into numerous folds or papillae interspersed with clefts (Fig. 2.4C). Not infrequently small bluish-gray bubbles and polyps are visible within the canal (Figs. 2.5 and 2.6). The lumen of the cervix ranges between 3 and 10 mm in diameter, depending on individual variation and parity. There is, however, some resiliency to light pressure that may allow 1 to 2 mm additional space with stretching. During stretching, the mucosal folds appear flat and white. During contact and low-pressure CO2 or liquid panoramic hysteroscopy, the pink papillary mucosal pattern with its plentiful fine, branched vessels is appreciated. However, with higher CO2 pressure, the endocervical canal appears as a flat, white cylindrical structure because the mucosal pattern has been smoothed and the vasculature occluded.
The isthmus is a flattened, narrowed, short canal between the upper portion of the cervix and the corpus. The mucosa is smooth compared with the highly folded endocervix. The isthmus measures about 1 cm in length and is marked by a construction (internal os) where it meets the cervix. The isthmus is very narrow in the nulliparous woman, but expands to approximately 1 cm after delivery.
The corpus forms the main mass of the uterus and is usually bent anteriorly on the isthmus and typically is tipped slightly to the right. The convex posterior wall of the uterus is covered with peritoneum (Fig. 2.7A). Two thirds of the flattened anterior aspect is covered with peritoneum as it reflects off the urinary bladder (Fig. 2.7B). The walls are heavily musculatured and measure about 2 cm thick.
The anterior and posterior walls of the uterus are in close apposition and are best appreciated in the natural state during contact hysteroscopy (Fig. 2.8A, B). The uterine cavity is most accurately described as potential. The potential cavity of the uterus is flattened and has the shape of an inverted triangle, with the base formed by a line drawn between the two tubal ostia and the apex at the isthmic opening. From top to bottom, this space measures 4 to 5 cm (Fig. 2.9). Hysterovolumetric studies of the uterus have been reported by Davis and Israel. The volume of fluid filling the cavity approximates 5 to 12 cc.
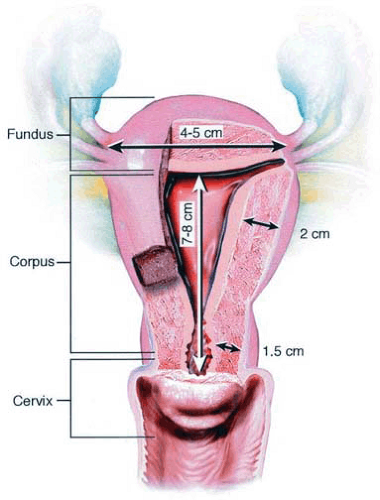 FIGURE 2.1 The anterior wall of the uterus has been cut out. The three major subdivisions of the uterus are clearly identified: cervix, corpus, and fundus. The thickest musculature is seen in the corpus and fundus. The narrowed area between the internal os of the cervix and the wider corpus is the isthmus. |
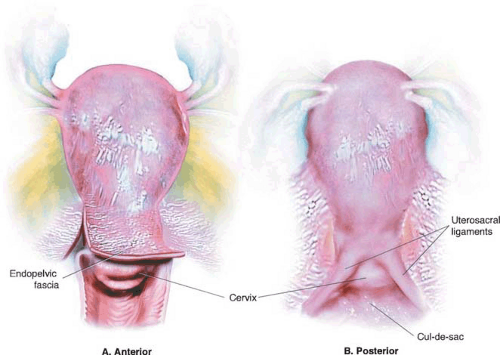 FIGURE 2.2 The cervix measures approximately 2.5 cm in height. Anteriorly (A) the cervix is separated from the bladder by the endopelvic fascia (arrow). Posteriorly (B) the cervix lies below the uterosacral ligaments and is covered with peritoneum, which reflects off the posterior vagina (cul-de-sac). |
The mucosa of the corpus (i.e., the endometrium) varies in thickness depending on the phase of the menstrual cycle and ranges between 1 and 8 mm. On gross examination it appears smooth and orange-tan and is usually thickest in the fundus (Fig. 2.10).
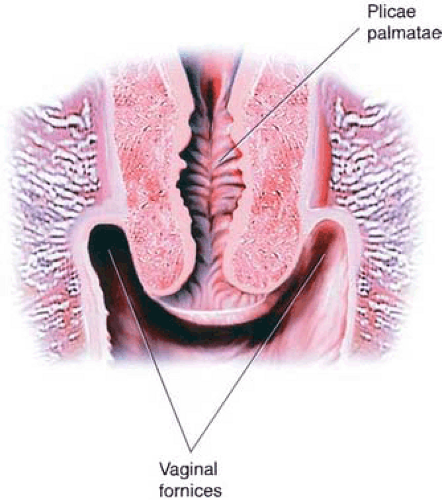 FIGURE 2.3 The cervix projects into the vagina in a slightly posterior direction. The external os is evident. The upper extent of the vagina is divided into four fornices. |
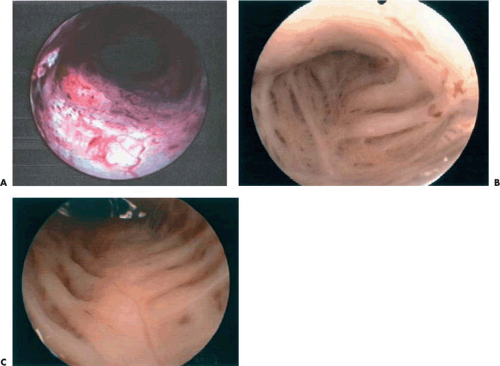 FIGURE 2.4 A: Hysteroscopic panoramic view of the cervical canal taken from the distal portion of the endocervix. B: Close-up view of endocervical canal showing plicae palmatae. C: The endocervix consists of numerous folds and clefts (glands). |
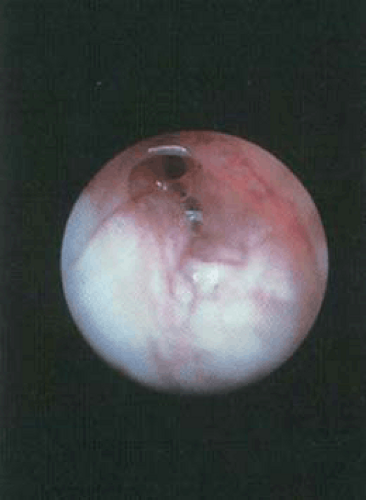 FIGURE 2.5 The endocervical mucosa os seen in panoramic hysteroscopy shows numerous folds and clefts. The mucosa is light pink and usually fills the area around the internal os. |
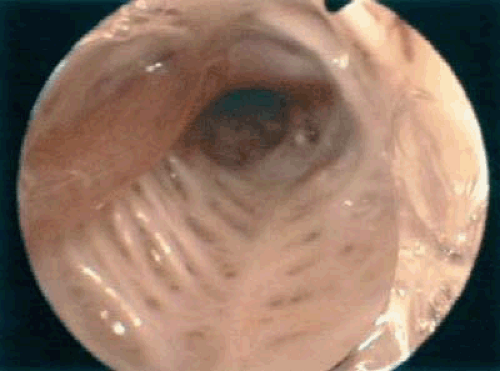 FIGURE 2.6 A thin endocervical mucosal polyp is seen arising high on the anterior cervical wall (red). |
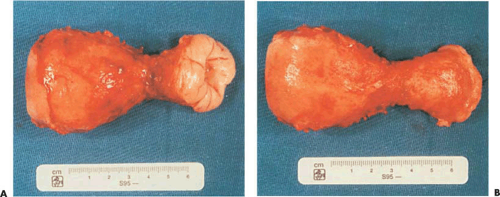 FIGURE 2.7 A: The anterior aspect of the uterus is flat tened. Two thirds of its surface is covered with peritoneum, which reflects from the upper portion of the urinary bladder. B: The convex posterior wall of the uterus is covered with peritoneum.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





