14
An Overview of Erectile Dysfunction in Aging Men
Case Histories
Case 1
A 55-year-old man with mild hypertension and coronary heart disease presented with erectile dysfunction (ED). Current medications included antihypertensives and nitrates. He had been counseled not to take sildenafil (Viagra) because of a positive chemical stress test. He was therefore tried on apomorphine (Uprima), unfortunately without a satisfactory outcome. Self-injection of prostaglandin E1 (PGE1) worked for him but he wanted to be rid of frequent injections and was opposed to getting a formal penile prosthetic implant. Finally, he had a Brindley penile autoinjector implant, which works by delivering a metered quantity of sodium nitroprusside into the corpora cavernosum after executing the tiny pump embedded into the central part of the scrotum. Each refill done percutaneously via a hypodermic needle permits 50 erections before the next visit to the urologist. This “implant” does not damage the corpus cavernosum like the classic implant. If so desired it can be explanted and the penis can be returned to the original preimplant status. It also does not preclude use of the other methods after it is removed.
Case 2
A 67-year-old man came for ED therapy in the andrology clinic. The use of Viagra restored his erections, but his wife refused to have intercourse with him, saying that she was menopausal, that her sex life was over, and that he must likewise accept the inevitable gracefully and not seek artificial rejuvenation. He gave up trying to reason with her, and sought gratification from prostitutes. His wife found out and came to the doctor’s office demanding the doctor refrain from giving her husband Viagra.
Case 3
A 30-year-old man was involved in a motor vehicle accident. He fractured his pelvis and could not produce a good erection. Neurological examination showed no focal deficits. Investigations included a color Doppler ultrasound, which showed an arteriogenic cause. Arteriography revealed damage to the artery in Alcock’s canal and no flow into the right deep cavernosal artery. A revascularization procedure using the inferior epigastric artery with microvascular anastomosis of the latter to the deep dorsal vein of the penis (arterialization of the deep dorsal vein of the penis) restored his erections to premorbid level of performance.
Introduction
An erection is a complex, involuntary, neuropsychological, hormone-mediated vascular event that occurs when blood rapidly flows into the penis and becomes trapped in its spongy chambers. Erectile dysfunction, the preferred term for impotence, was defined at the National Institutes of Health Consensus Conference, December 1992, as “the inability to achieve or maintain an erection satisfactory for sexual intercourse.” Satisfaction is determined by both patient and partner, making erectile dysfunction a “couple’s disease.”
For a man, however, sexual performance carries an identity and the sense of self-esteem in his society and the world. Thus sexual performance in the man has unprecedented importance, depending on the erectile function of the male sex organ. Potentially, ED plays an adverse role in human procreation, as male infertility may also be a consequence. In daily life, it is very easy for men to admit having a sore throat or hemorrhoids. However, admitting to having ED is difficult for the male ego, especially if the dysfunction occurs at a younger age.
The Physiology and Mechanism of Penile Erection
Coordinated control of psychological, hormonal, neurological, vascular, and cavernosal events results in an erection. An erection of the penis is a hemodynamic event, influenced by relaxation of smooth muscle cells in the corpora cavernosa and the arteries of the penis, coincident with restriction of penile venous outflow.1,2 The arterial blood flow into the penis is therefore increased, by way of the cavernosal arteries and the helicine arteries, which deliver blood directly to the cavernosal spaces.1 There is consequently a sustained elevation of the intracavernosal arterial pressure with relaxation of smooth muscle trabeculae and pooling of blood within the corpora cavernosa, leading to engorgement of cavernosal tissue and finally to penile erection.1
The relaxation of smooth muscle cells in the corpora cavernosa is mediated by 3’5′-cyclic guanosine monophosphate (cGMP). This critical event is brought about by nitric oxide (NO).2,3 The response to a sexual stimulus is the release of NO at the nonadrenergic, noncholinergic nerve endings innervating the penile arterioles, leading to the relaxation of smooth muscle cells.3 Subsequently, cGMP is hydrolyzed by a cGMP specific phosphodiesterase-5 (PDE-5) isoenzyme, which is richly present in the cavernosal tissues of the penis.1 Besides the NO system, relaxation of cavernosal smooth muscle is also initiated by other neurotransmitters including acetylcholine, vasoactive intestinal polypeptide (VIP) via the VIP-ergic system, prostaglandin via the prostacyclin system, and NO via the nitrergic system.
Definition and Prevalence of Erectile Dysfunction
Erectile dysfunction (ED) is one form of the sexual dysfunction that leads to the patient’s experience of inadequate libido, inefficient orgasm, and retarded or premature ejaculation. In recent times, ED has been labeled as the most common sexual problem among pleasure-seeking males and a complaint of all men irrespective of their age, race, and culture. It is reported that nearly 100 million men around the world are experiencing ED, but only 10 million are opting for treatment, despite enormous advancements and treatment facilities in all parts of the world. To cite a few countries, in China and Korea only 9% and 30% of men, respectively, voluntarily admit to having ED, and in most of the other countries in Asia it is still considered a very sensitive issue with considerable social stigma.
Age-Specific Incidence
The incidence of ED is reported to be associated with increasing age. In the United States, the Massachusetts Male Aging Study (MMAS) reported that 5% of men at 40 years, and 15% of men at 70 years are suffering from complete ED. The prevalence of some degree of ED is reported as 52% of men for the age range 40 to 70 years, of which 25% are of moderate extent and 10% complete.4 The risk of ED in this cohort of men was 26 cases per 1000 men annually. The annual incidence rate increased with each decade: from 12.4 cases per 1000 man-years in men between 40 and 50 years to 46.4 cases in men between 50 and 60 years. As a result, some men consider this is as an evil, whereas others consider it as a necessary evil (unavoidable aging process). More recently many young men were also found to have ED; however, the problem is more significant after the age of 50 (Fig. 14–1).5 Marital status also influences the incidence of ED. Symptoms of ED are significantly higher in unmarried men than in married men.6
What Causes Erectile Dysfunction?
Many men believe that ED is the result of stress or anxiety or a direct impact of aging. However, it is also caused by various other comorbid conditions such as diabetes mellitus (DM), heart disease, hypertension, and penile diseases. In addition, other causes such as levels of testosterone, high-density lipoprotein, peptic ulcer, arthritis, alcohol abuse, drug abuse, smoking, and allergy are also associated with ED. Stroke, spinal cord disorders, temporal lobe epilepsy, urinary tract symptoms, and multiple sclerosis might also lead to erectile dysfunction.6,7 Further, medications for other common problems could be causative and cannot be neglected as an important contribution to this malady, for example in outpatient clinics, around 25% of ED was diagnosed as drug-mediated. Among these drugs, the prime agent is thiazide diuretics followed by β-blockers.8 These drugs either reduce blood pressure or act on the smooth muscles of the corpus cavernosa. Other drugs such as benzodiazepines, serotonin inhibitors, cimetidine, digoxin, and metoclopramide would also increase ED.9 In untreated depressions, 20 to 40% prevalence of ED has been reported, and its severity was found to increase with the magnitude of depression. In men over age 50, myocardial infarction and vascular disorders such as insufficient arterial inflow and excessive venous outflow account for ∼50 and 64% of ED, respectively10,11 As diabetes and cardiovascular diseases are common in men with ED, we will briefly concentrate on the association of ED with these two diseases. The etiology of ED is summarized in Table 14–1.
Erectile Dysfunction in Diabetes
In diabetic patients ED is very common.11 Of late, the number of diabetic patients is on the rise and as a result 30% of ED in Singapore is attributed to diabetes.12 In the Western world the situation is not so conspicuous with diabetes, where only 25% of ED is associated with diabetes. Moreover, with an increase in age and diabetes the problem of ED becomes compounded (Fig. 14–2).13 Because of this potential effect of diabetes on ED, diabetes can also be regarded as a potential diagnostic indicator of ED in men.
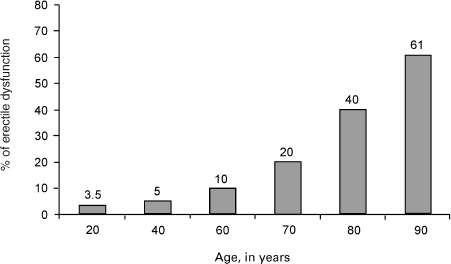
FIGURE 14-1. Incidence of erectile dysfunction by age.
Hypogonadism and diabetes has a cumulative effect on the erectile function through their role in changing the ability of endothelial cells to produce neurotransmitters and thus cause ED. An Italian study assessed the prevalence of ED in 1383 men with type 1 DM and in 8373 men with type 2 DM, between the ages of 20 and 69 years.14 Not unexpectedly, age was a factor in the prevalence, but taking age into account 37/100 men with type 2, and 51/100 with type 1 DM had erectile problems. Romeo et al15 established that rather than age, glycemic control and peripheral neuropathy were independent predictors of ED.
Erectile Dysfunction in Cardiac Patients
Erectile dysfunction is a common condition in men with cardiovascular disease. Some men realize that there is a degree of cardiac risk associated with sexual activity, which subsequently becomes a concern for many patients with cardiovascular disease, particularly those who have experienced acute cardiac events in the past. The relative risk of an incidence of myocardial infarction following sexual activity was no different in patients with a previous history of myocardial infarction or angina pectoris than in patients with no history of cardiovascular disease.16,17 ED is also often associated with cardiovascular diseases requiring drug treatment. The medications for these conditions are reported to cause or contribute to ED at a rate of 25%.8 Also, medications such as antidepressants and luteinizing-releasing hormone analogs may be responsible for ED, too. Hormonal changes such as age-related decline in testosterone and even more so of free testosterone level and other hormonal disorders, such as hypo- and hyperthyroidism, are reported to result in ED.18,19
| Vascular disease affecting large or small vessels |
| Endocrine disorders (e.g., pituitary problems, gonadal failure, adrenal disorders, thyroid disorders, diabetes mellitus) |
| Local factors (e.g., cavernous veno-occlusive dysfunction) |
| Poor overall health (e.g., severe angina or shortness of breath that limits or prevents the physical act of intercourse) |
| Smoking and consumption of alcohol |
| Medication use (see text for examples) |
| Inflammatory conditions of the prostate (e.g., prostatitis), urethra, or seminal vesicles |
| Surgical procedures (e.g., perineal surgery, radical prostatectomy, cystoprostatectomy, abdominal-perineal resection, vascular surgery) |
| Pelvic fractures with or without urethral distraction injuries |
| Lumbar neurological injuries |
| Neurological conditions (e.g., Parkinson’s disease, amyotrophic lateral sclerosis, multiple sclerosis, tabes, peripheral neuropathies) |
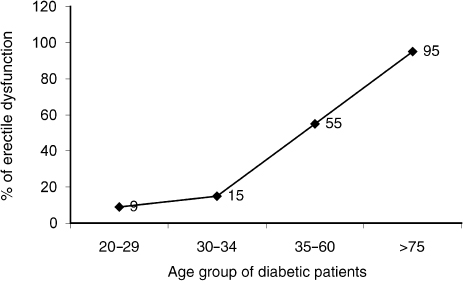
FIGURE 14-2. Incidence of erectile dysfunction in diabetic patients by age group. (Adapted from McCulloch DK, Campbell IW, Wu FC, Prescott RJ, Clarke BF. The prevalence of diabetic impotence. Diabetologia 1980;18:279–283, with permission.)
Despite several organic causes of ED, potential problems due to psychogenic causes cannot be overlooked. Of these, sexual fear, unsatisfactory interpersonal relationships, depression, identity problems and lifestyle, miseducation toward sex orientation, anxiety, shame or guilt, and past sexual history play an important role in men’s perception of sexual prowess and vigor.
Classification and Quantification of Erectile Dysfunction
Based on severity, etiology, and onset, ED is classified into three major categories: mild, moderate, and severe. From a clinical standpoint, the patient’s physical and biochemical assessment variables should be considered for proper classification.
Mild ED is defined as a decreased ability to attain and or maintain an erection with intermittent satisfactory sexual performance.
Moderate ED is regarded as a decreased ability to attain and or maintain an erection with infrequent satisfactory sexual performance.
Severe ED is meant as a decreased ability to attain and or maintain an erection with rare or absent satisfactory sexual performance.
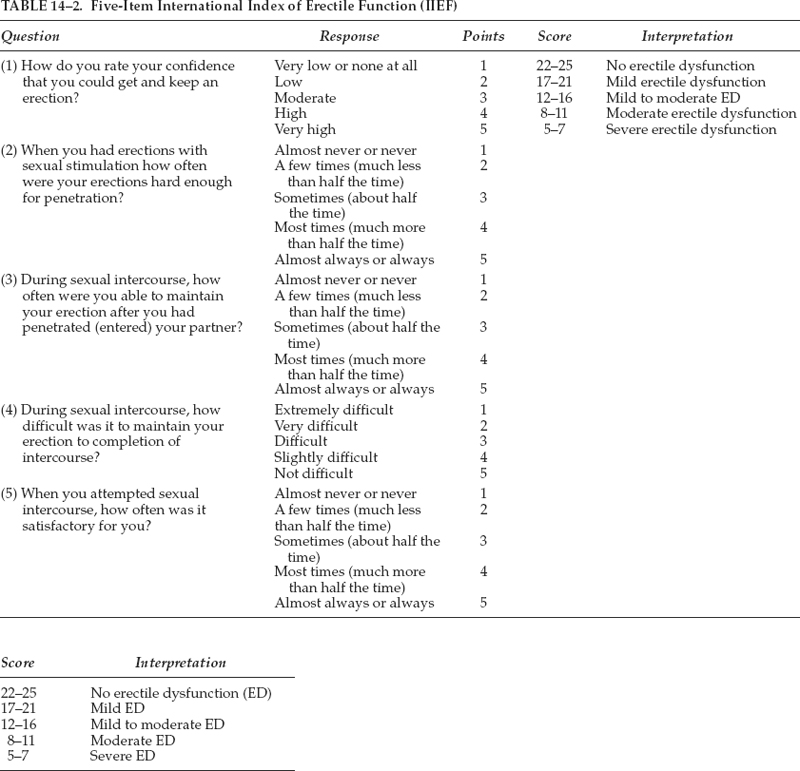
The 15-item questionnaire of the International Index of Erectile Function (IIEF) is used to quantify the degree of erectile function in men. It addresses and measures various attributes of sex, such as activity, intercourse, relationship, desire, sexual satisfaction, and stimulation. An abbreviated five-item questionnaire is also available (Table 14–2).
How Can We Investigate ED?
In most instances, a careful history and physical examination is sufficient to evaluate a patient for ED. However, in certain unclear cases investigations are needed. These tests are often performed in clinical trials, so as to have objective outcomes, rather than those subjectively reported by the patient.
Pharmacological Testing
Office pharmacological testing is useful as it is offers information to the physician. The test involves intra-cavernosal injection of a small amount of an active agent [e.g., 10 µg of alprostadil (PGE1)] that, theoretically, would produce a normal or priapic erection in a patient with normal erectile function but a poor response in a patient with ED. The problem with this test is that unless the patient’s sympathetic nerve impulses are completely overcome by the injected agent, he may have a poor erection even though his erectile function is normal.
Hormonal Assays
Measuring serum levels of bioavailable, total and free testosterone, gonadotropins, and gonadotropin-releasing hormone may be helpful in a patient in whom history taking or physical examination suggests lack of androgen stimulation. Androgen insufficiency is not a direct cause of ED, but is often associated with ED. Features of hypogonadism include poor libido, a disproportionately small prostate gland relative to the patient’s age, small or soft testicles, and noticeable thinning or diminished growth of the beard. If the patient’s total testosterone level is low, the prolactin level should be checked to exclude a prolactinoma.
Nocturnal Studies
Nocturnal studies present perhaps a true picture of ED due to organic causes. The most complete evaluation of nocturnal erectile function is obtained in a sleep laboratory, where patients are monitored for rapid-eye-movement (REM) sleep. Under normal conditions, an erection would be expected to occur with each REM episode. The erection can be described in terms of tumescence and buckling force, which is a measure of rigidity.
Vascular Erectile Testing
Duplex Doppler ultrasonography has been used extensively. As the clinical evaluation is often sufficient, evaluation of erectile function with Doppler ultrasound may be useful for evaluating resistant cases of ED and treatment selection. Doppler studies provide information about both arterial and venous flow. Dynamic infusion caversometry and cavernosography (DICC) can also provide detailed data about pressure related to erectile function, but this information often is more extensive than is required for treatment of ED.
What Are the Treatment Modalities for Erectile Dysfunction?
Because ED is a multifactorial disorder, identifying the exact cause is of more importance than therapeutic intervention at the initial visit. Involving the female partner would also be helpful in circumventing ED. Moreover, a holistic approach using modern medications, surgery, or technology with a personalized touch could mitigate ED when considering the available options to achieve the desired goal. Several therapeutic medications and techniques have evolved to mitigate ED, of which, oral medications has become the first-line nonsurgical treatment option for many patients.20 Similarly, intracavernosal injections, microsurgical revascularization, and the implantation of penile prostheses21 have also gained significant attention among a broader group of patients who are affluent in society and nonresponsive to alternative treatment modalities.
The penile prosthesis is a rigid, hinged, mechanical, inflatable, or hydraulic structure used to mechanically overcome ED. Although penile prosthetic implants have been the treatment choice for many nonresponsive patients to alternative medications, proper diagnosis should be made to identify the cause of the ED in these patients. The clinical success of penile implant therapy depends on postoperative infection, the smooth and uncomplicated execution of the operation, avoidance of technical errors, the durability of the prosthetic material, and anatomic features of the penis,21 as complications arising from these factors often warrant removal of the prosthesis with the sequela of complete ED.
Some of the oral compounds used for ED are be-raprost, pinacidil, alprostadil, papaverine, phento-lamine, yohimbine, sildenafil, tadalafil, vardenafil, and apomorphine. At times, these treatments are unsatisfactory because of patient reluctance, unpredictable efficacy, inconvenience, and nonavailability, and inevitably they all lack spontaneity. When ED is remedied by pharmacological modalities, an adequate column of penile blood gives an erection of sufficient rigidity and duration for satisfactory sexual intercourse.4 We will briefly concentrate on widely prescribed and promising oral medicines for ED.
Sildenafil citrate (Viagra) is a selective phosphodiesterase-5 inhibitor and has been shown to be highly efficacious in men with ED originating from a wide variety of etiologies.20,22 It arrests the metabolic breakdown of cGMP. Compared with other oral agents Viagra has been identified as promising first-line treatment for ED because of its combined high efficacy with a good safety profile. Fig. 14–3 illustrates the clinical efficacy of Viagra compared with placebo in men with ED.
Viagra also has been proven to be effective in diabetic patients. Though many therapeutic agents are available for ED, proper diagnosis and medications are needed for sustained efficacy and durability of these treatments. Despite an increase in erection with Viagra, some of the side effects, such as arrhythmias, transient ischemic attacks, stroke, hypertension, headache, flushing, dyspepsia, and visual abnormalities, should be expected in those at risk and should be predetermined before prescription. One possible disadvantage of Viagra is the interaction with food and shorter half-life. However, the clinical experience with Viagra is unparalleled, with several million men worldwide using this drug.
Tadalafil (Cialis) or IC351 is a new representative compound of the second generation of selective phosphodiesterase-5 (PDE-5) inhibitors.23 The selectivity ratio versus PDE-5 is more than 10,000 for PDE-1 through PDE-4 and PDE-7 through PDE-10 and 780 for PDE-6. In the European daily-dosing trial, the efficacy rates were up to 93% for successful intercourses with completion in the 50-mg dose in patients with mild to moderate ED. In two different dose-ranging studies with 2 to 25 mg taken as needed, efficacy rates of up to 88% improvement in erections and up to 73% successful intercourses with completion were achieved. In a placebo-controlled, fixed-dose (10- and 20-mg) trial in diabetic patients, improved erections of 56% and 64% were reported compared with 25% after placebo. Drug-related adverse effects, with headache in up to 23% of patients (placebo, up to 17%), dyspepsia in up to 11% (placebo, up to 7%), back pain in up to 4.7% (placebo, 0%), and myalgia in up to 4.1% (placebo, up to 2.4%), were mostly mild to moderate. Neither drug-related serious cardiovascular adverse events nor color vision disturbances were encountered. The long half-life (>17 hour), with a comfortably long window of opportunity, releases couples from the need to plan sexual activities and therefore provides the highest amount of spontaneity for sexual activities.
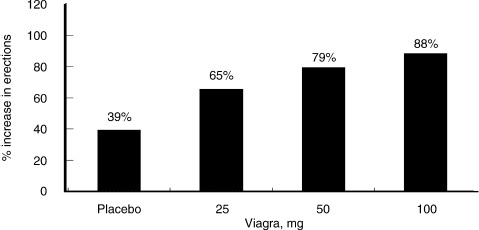
FIGURE 14-3. Increase in erections as a response to increasing dosages of sildenafil (Viagra). (Adapted from Goldstein I, Lue TF, Padma-Nathan H, Rosen RC, Steers WD, Wicker PA. Oral sildenafil in the treatment of erectile dysfunction. N Engl J Med 1998;338:1397–1404, with permission.)
Vardenafil (Levitra) selectively inhibits PDE-5, an enzyme that hydrolyzes cyclic guanosine monophosphate in the cavernosum tissue of the penis.24 Inhibition of PDE-5 results in increased arterial blood flow leading to enlargement of the corpus cavernosum. Because of the increased tumescence, veins are compressed between the corpus cavernosum and the tunica albuginea, resulting in an erection. Vardenafil has a high bioavailability and is rapidly absorbed. An erection of >60% rigidity was maintained for approximately twice as long following visual stimulation in patients treated with vardenafil 10 or 20 mg than in recipients of placebo. In a large, placebo-controlled trial in patients with mild to severe ED, vardenafil 5, 10, or 20 mg taken as needed over a 12-week period significantly improved the scores in questions 3 and 4 of the International Index of Erectile Function (IIEF). The rate of successful attempts at intercourse with ejaculation was also significantly higher with vardenafil (71 to 75%) than in the placebo group (39.5%), and significantly more patients treated with vardenafil than placebo responded “yes” to a Global Assessment Questionnaire (GAQ) asking if treatment had improved erections. In a 26-week trial in 736 men with ED of varied etiologies and severity, patients receiving vardenafil 5, 10, or 20 mg experienced significantly improved erections, with 85% of the vardenafil 20 mg recipients reporting improved erectile function (assessed using the GAQ) compared with 28% of placebo recipients. Treatment with vardenafil also significantly improved scores in response to questions 3 and 4 of the IIEF compared with placebo. A 12-week trial in 452 men with ED associated with diabetes mellitus demonstrated that treatment with vardenafil 20 mg compared with placebo significantly improved IIEF erectile function domain scores and the rate of positive responders to the erectile improvement GAQ. Similar results were reported in a placebo-controlled trial of vardenafil 10 to 20 mg involving 440 patients with ED after radical prostatectomy. Adverse events associated with vardenafil were those commonly associated with PDE-5 inhibitors: headache, flushing, dyspepsia, and rhinitis. These were mostly dose-dependent and mild to moderate in intensity.
Apomorphine SL (Ixense; Uprima) is a new oral medication shown to be effective in the treatment of ED.25 This compound is a dopaminergic agonist with affinity for dopamine receptor sites—mostly D(2)—within the brain known to be involved in sexual function. Apomorphine induces selective activation in the nucleus paraventricularis leading to erectogenic signals. More than 5000 men with ED participated in phase II/III clinical trials assessing the safety and efficacy of doses ranging from 2 to 6 mg. The most favorable risk/benefit ratio is seen with a dose-optimization regimen of 2 to 3 mg: the 3-mg dose provides efficacy comparable to that of 4 mg but with fewer side effects. Consequently, review of clinical studies focuses on data with the 2- to 3-mg dose, the registered dose for use in clinical practice. The primary efficacy end point in most clinical trials with apomorphine SL was the percentage of attempts resulting in erections firm enough for intercourse—one of the most rigorous end points used in ED trials to date. These data were collected from both patients and their partners by reviewing entries in patient diaries and partner Brief Sexual Function Inventory (BSFI) questionnaires. Secondary end points included percentage of attempts resulting in intercourse and improvement in ED severity based on the IIEF. The proportion of attempts resulting in erections firm enough for intercourse was 49.4% with 3 mg compared with the baseline value of 24.3%. Partner evaluations corresponded with those of the patients. Erections occurred between 18 and 19 minutes after taking apomorphine SL 2 or 3mg. The most common side effect was nausea, which declined with continued use. Vasovagal syncope was reported in <0.2% of men, and was preceded by clear prodromal symptoms. Apomorphine SL is also an effective, well-tolerated drug for ED.
Discussion of the Case Histories
Case 1
The desperate patient fearful of the traditional implant can now use the latest prosthesis invented by Prof. Giles Brindley from the University of London. It is excellent for neurogenic ED, mild to moderate venogenic ED, some cases of arteriogenic ED, and most cases of psychogenic ED. If PGE1 works, then this method will most certainly be effective.
Case 2
Couple counseling is vital as exemplified by the events of this case. The practitioner should try at all costs to get the couple to see how the two parties must interact, and to educate both on sexual health concerns that apply today even for the old and the elderly. In this era of the availability of countless varieties of erectogenic drugs and increasing awareness of female sexuality and female sexual dysfunction, couple concerns and couple therapy have an increasingly vital role to play in sexual medicine.
Case 3
Acute vascular injuries respond well to revascularization procedures in the younger individual. Middle-aged and older men will have a fairly rapid relapse with arterializations procedures because of higher thrombosis rates occurring at the site of microvascular anastomosis in this cohort. Hence we recommend this procedure only to younger men.
Conclusion and Key Points
Erectile dysfunction has become more widely accepted as a disease entity, and treatment should be targeted not only on improving the quality of life, but also on the associated disease states.26 In terms of numbers, prevalence studies suggest that one in two men over 50 years have an associated ED.
• ED is associated with comorbid states including diabetes mellitus, heart disease, hypertension, etc.
• ED is often associated with hypogonadism and the andropause syndrome. Although hypogonadism does not directly lead to ED, treatment with testosterone is supplementary as well as complementary.
• Some medications can lead to ED, and the practitioner should adjust or remove these medications before adding PDE-5 inhibitors, for instance.
• It is important to objectively classify the stage of ED in the assessment of treatment success or failure.
• Newer oral medication for treatment of ED will mean more patients appearing for treatment, and hence an opportunity to screen for comorbid disorders.
REFERENCES
1. Andersen KE, Wagner G. Physiology of penile erection. Physiol Rev 1998;75:191–236
2. Naylor AM. Endogenous neurotransmitters mediating penile erection. Br J Urol 1998;81:424–431
3. Rajfer J, Aronson WJ, Bush PA, Dorey FJ, Ignarro LJ. Nitric oxide as a mediator of relaxation of the corpus cavernosum in response to nonadrenergic, noncholinergic neurotransmission. N Engl J Med 1992;326:90–94
4. Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosexual correlates: results of the Massachusetts Male Aging study. J Urol 1994;151: 54–61
5. Kaiser FE. Erectile dysfunction in the aging man. In: Kaiser FE, ed. The Medical Clinics of North America: The Aging Male Patient. Philadelphia: WB Saunders; 1999:1267–1278
6. Laumann EO, Anthony Paik MA, Raymond RC. Sexual dysfunction in the United States: prevalence and predictors. JAMA 1999;281:537–544
7. Kaiser FE. Sexuality and impotence in the aging man. Clin Geriatr Med 1991;7:63–72
8. Buffum J. Prescription drugs and sexual function. Psychiatr Med 1992;10:181–198
9. Burchardt M, Burchardt T, Baer L, et al. Hypertension is associated with severe erectile dysfunction. J Urol 2000;164: 1188–1191
10. Lue TF, Hricak H, Schmidt RA, et al. Functional evaluation of penile veins by cavernosography in papaverine induced erection. J Urol 1986;135:479–482
11. Kaiser FE, Korenmann SG. Impotence in diabetic men. Am J Med 1988;85:147–152
12. Lim PH, Li MK, Ng FC, et al. Clinical efficacy and safety of sildenafil citrate (Viagra) in a multiracial population of Singapore: a retrospective study of 1520 patients. Int J Urol 2002;9: 308–315
13. McCulloch DK, Campbell IW, Wu FC, Prescott RJ, Clarke BF. The prevalence of diabetic impotence. Diabetologia 1980;18: 279–283
14. Fedele D, Bortlotti A, Coscelli C, et al. Erectile dysfunction in type 1 and 2 diabetics in Italy. Int J Epidemiol 2000; 29:524–531
15. Romeo JH, Seftel AD, Madhun ZT, Aron DC. Sexual function in men with diabetes type 2: association with glycemic control. J Urol 2000;163:788–791
16. Muller JE, Mittleman A, Maclure M, Sherwood TB, Tofler GH. Triggering myocardial infarction by sexual activity. Low absolute risk and prevention by regular physical exertion. JAMA 1996;275:1405–1409
17. De Busk RF. Sexual activity triggering myocardial infarction. One less thing to worry about. JAMA 1996;275:1447–1448
18. Blackman MR, Kowatch MA, Wehmann RE, Harmann SM. Basal serum prolactin levels and prolactin responses to constant infusions of thyrotropin releasing hormone in healthy aging men. J Gerontol 1986;41:699–705
19. Foster RS, Mulcahy JJ, Callagher JT, Crabtree R, Brashear D. Role of serum prolactin determination in evaluation of impotent patient. Urology 1990;36:499–501
20. Goldstein I, Lue TF, Padma-Nathan H, Rosen RC, Steers WD, Wicker PA. Oral sildenafil in the treatment of erectile dysfunction. N Engl J Med 1998;338:1397–1404
21. Rosen JC. Erectile dysfunction: the medicalization of male sexuality. Clin Psychol Rev 1996;16:497–519
22. Perrin J. And then came Viagra. Pharmaceu J 1998;260:707
23. Porst H. IC351 (tadalafil, Cialis): update on clinical experience. Int J Impot Res 2002;(suppl 1):S57–S64
24. Ormrod D, Easthope SE, Figgitt DP. Vardenafil. Drugs Aging 2002;19:217–227
25. Altwein JE, Keuler FU. Oral treatment of erectile dysfunction with apomorphine SL. Urol Int 2001;67:257–263
26. Jordan GH. Erectile function and dysfunction. Postgrad Med 1999;105:131–134
< div class='tao-gold-member'>
Related posts:
 Bioidentical Hormone Replacement with Testosterone in Men
Bioidentical Hormone Replacement with Testosterone in Men
 Effect of Androgens on Muscle, Bone, and Hair in Men
Effect of Androgens on Muscle, Bone, and Hair in Men
 Androgens and Sexuality in Aging Men
Androgens and Sexuality in Aging Men
 Preventive Gerontology in Men’s Health: Optimal Aging Concepts for Midlife and Beyond
Preventive Gerontology in Men’s Health: Optimal Aging Concepts for Midlife and Beyond
 Alzheimer’s Disease in Older Men: Are There Gender-Specific Etiological Issues and Treatments?
Alzheimer’s Disease in Older Men: Are There Gender-Specific Etiological Issues and Treatments?
 Prostate Cancer: Controversies and Developments in Screening and Treatments
Prostate Cancer: Controversies and Developments in Screening and Treatments



