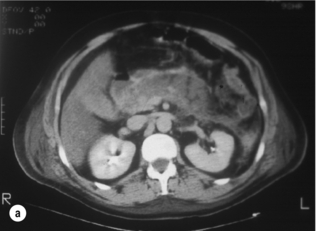
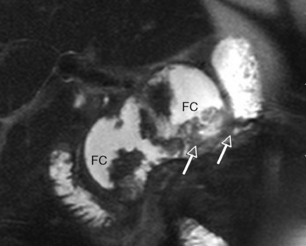
13 Acute pancreatitis is a common cause for emergency hospital admission, with approximately 40 cases per year for each 100 000 population in Scotland,1 Norway2 and Sweden.3 There has been a steady increase in the incidence and a slight reduction in case mortality, although not population mortality, over the past 45 years.4 In approximately 80% of patients, acute pancreatitis is a rapidly-resolving condition requiring little more than analgesia and a short period of intravenous fluid resuscitation, with the remainder developing a multisystem illness characterised by a systemic inflammatory response with a variable degree of organ dysfunction. Experimental models have shed some light on the mechanism by which pancreatic duct obstruction induces acute pancreatitis. Changes in the pattern of enzyme secretion within pancreatic acinar cells, coupled with intracellular zymogen activation, are considered the important early events in the development of acute pancreatitis. Disruption of the paracellular barrier allows release of pancreatic enzymes into the paracellular space. Inflammatory cells and inflammatory mediators may further exacerbate the acinar cell injury.4 Research has shown that many of these early events can be triggered by an increase in intracellular calcium.5 The mechanism of alcohol-induced acute pancreatitis is less clear, but alcohol has been shown to increase the sensitivity of acinar cells to cholecystokinin hyperstimulation, resulting in enhanced intracellular protease activation.6 Alcohol also influences acinar cell calcium homeostasis, but several alternative theories have been proposed. Acute pancreatitis varies from a mild, self-limiting attack to a severe life-threatening illness and, for this reason, patients are often classified as having either mild or severe acute pancreatitis (see Box 13.1). This rather simplistic description ignores the wide variety of clinical behaviour that can be observed in these patients but helps to focus attention on the subgroup of patients who develop complications. Currently, the internationally accepted classification of acute pancreatitis and its complications is set out in the paper arising from the Atlanta Conference.7 Improved understanding of treatment concepts and the dynamic nature of the pathophysiology has rendered a number of the concepts outlined in the Atlanta Conference outdated and a revision has recently been published.8 Within this framework different patterns of disease have emerged. Multicentre trials in acute pancreatitis have enabled prospective study of severe acute pancreatitis and several important points have emerged. Firstly, the majority of patients who develop severe acute pancreatitis have evidence of early systemic organ dysfunction.9 It is exceptional for a patient to have no evidence of organ failure in the first week of illness and to subsequently develop a significant late local complication. Secondly, most patients who develop organ failure have evidence of this at the time of admission or very shortly thereafter.10 Thirdly, while the tendency is for early organ dysfunction to recover without further problems, worsening organ failure is associated with a high mortality.9,11,12 The majority of patients with severe early organ dysfunction will have pancreatic necrosis on computed tomography (CT) scan. A significant proportion (30–40%) of patients with pancreatic necrosis will develop secondary pancreatic infection, usually in the second to third week after admission,13 which may be associated with a deterioration in organ failure. Patients who have infected pancreatic necrosis complicated by multiple organ failure represent a formidable management challenge. In the majority of patients the diagnosis of acute pancreatitis is relatively easy, characterised by a clinical presentation of sudden severe epigastric pain radiating through to the back. Vomiting within the first 24 hours is very frequently severe and contributes to dehydration. Other signs and symptoms such as tachycardia, tachypnoea and circulatory collapse are dependent on the severity of the attack. A raised serum amylase (at least three times the upper limit of normal) supports the diagnosis in >95% of cases. Serum amylase estimation may be inaccurate in association with hyperlipidaemia, where a raised urinary amylase can be diagnostic. Serum lipase may be marginally more accurate but is not commonly available in routine clinical practice. CT can confirm the diagnosis where doubt exists, or in patients with delayed presentation, and it should therefore be very uncommon for the diagnosis to be made at laparotomy (Fig. 13.1). Genetic familial defects of the cationic trypsinogen gene14 (N29I, RII7H) and the cystic fibrosis gene (CTFR) may be associated with recurrent pancreatitis, but severe acute inflammatory changes are uncommon. Drug-induced acute pancreatitis may occur following ingestion of a number of drugs;15 those most commonly implicated are valproic acid, azathioprine, L-asparaginase and corticosteroids. However, unless gallstone disease has been excluded with confidence it is unwise to ascribe acute pancreatitis to a particular drug. Repeat exposure to the same drug again causing acute pancreatitis is the strongest evidence of a direct association. Autoimmune pancreatitis is a rare condition, considered part of the IgG4-related autoimmune disease spectrum.16 This presents as abdominal pain associated with homogeneous gland enlargement with a well-defined edge on CT, an increased IgG4/IgG ratio and a periductal lymphoplasmocytic infiltrate on biopsy. This may also be associated with abnormalities in the extrahepatic biliary tree resembling sclerosis cholangitis and a response to steroids is diagnostic. Focal autoimmune pancreatitis may prove difficult to differentiate from carcinoma. There are established associations with other autoimmune diseases (polyarteritis nodosa, systemic lupus erythematosus, vasculitis) and inflammatory bowel disease (Crohn’s and ulcerative colitis), and many are now considered part of the autoimmune spectrum, although only a small proportion appear to have an association with IgG4 serum or tissue abnormalities. Sphincter manometric abnormalities Type 1 pancreatic sphincter dysfunction17 may be associated with hyperamylasaemia and abnormalities on sphincter manometry, as part of a global gut dysmotility spectrum. Managament of sphincter spasm may only partly resolve the patient’s symptoms. Conventional treatment involves endoscopic sphincterotomy, but the risk of post-ERCP pancreatitis in these patients is high (30%). The dynamic nature of organ dysfunction in patients presenting with acute pancreatitis has been well described,9 and for over 30 years authors have explored ways of ‘predicting’ those patients with more severe disease. Overall mortality, whether early or late, is also associated with the development and persistence of organ failure.18 This was indirectly shown, if not recognised, 25 years previously with the development of the predictive multifactorial scoring systems – Ranson,19 Glasgow20 and APACHE II21 – which, rather than predicting the subsequent development of organ failure, more accurately identified established multisystem organ dysfunction. Their principal use is to remind the inexperienced of the multisystem nature of the disease process, or as a method of stratifying patients within a study protocol. Of the multiple factor scoring systems, APACHE II provides the best prediction of mortality but the mainstay of assessment remains repeated, careful clinical observation.22 The most widely studied single predictive marker is serum CRP. The major advantage of CRP is its routine availability in clinical practice. Patients with clinically severe pancreatitis usually have a CRP > 200 mg/L, with a practical cut-off being 150 mg/L, but its serum peak is not reached for 36–48 h. The positive predictive value of CRP is similar to that of APACHE II22 but its major use is in monitoring the clinical course during the acute and recovery phase. Peak levels of interleukin-6 (IL-6) occur within 24 h and this has aroused interest in its use as a predictor of outcome. IL-6 is a pro-inflammatory cytokine induced by stimuli such as tumour necrosis factor (TNF) and interleukin-1 (IL-1). Other single predictive markers that have been studied include trypsinogen activation peptide (TAP), leucocyte polymorph neutrophil (PMN) elastase, TNF and serum procalcitonin. Procalcitonin is the precursor of the hormone calcitonin and is raised in the presence of an inflammatory response, particularly where this is bacterial in origin. Serum procalcitonin is a promising marker of both severe acute pancreatitis and of infected pancreatic necrosis in the later phase.22,23 IAH is recognised as a contributing factor to organ dysfunction in the context of a variety of acute abdominal processes. Most of the literature to date focuses on trauma patients, but there is increasing interest in its role in patients with severe acute pancreatitis (SAP). There are data to suggest that raised intra-abdominal pressure (IAP) may be associated with disease severity,24 organ failure and mortality in SAP.25 There are, however, no data to suggest improved outcome following surgical decompression for raised IAP in acute pancreatitis, and indeed this may be harmful. At present the monitoring of IAP cannot be recommended outside of a clinical trial. All patients with acute pancreatitis should have an ultrasonic assessment of the biliary tree within 24 h of admission.26 All patients with acute pancreatitis should have an ultrasonic assessment of the biliary tree within 24 h of admission.26 In those with gallstones, the majority will have mild disease, and this will facilitate definitive treatment of cholelithiasis prior to discharge. In the emergency situation, ultrasonography can be difficult due to a number of factors, including the presence of intraluminal bowel gas or lack of patient cooperation. Therefore, in patients with a negative initial US, and no other obvious aetiological factor, the US should be repeated prior to discharge before excluding gallstones as a potential aetiological factor. The main role of CT in the early phase of acute pancreatitis is to clarify the diagnosis in cases where there is diagnostic uncertainty. In patients with severe acute pancreatitis, particularly when complicated by MODS, early CT helps to exclude other pathology such as intestinal perforation, gut ischaemia or dissecting aortic aneurysm. Dynamic contrast-enhanced CT can also be used to assess disease severity (Fig. 13.2) and predict the potential for complications.27 Although not widely used for this purpose clinically in the UK, it is routinely used in many other countries, and can be useful for stratification of patients in clinical trials. The CT Severity Index (CTSI)27 combines a score for the radiological pancreatic and peripancreatic abnormalities with a weighting for the extent of necrosis. More recently there are reports of perfusion CT, which may be a useful modality for detecting early, subclinical ischaemic changes in the pancreas that then lead to pancreatic necrosis. Magnetic resonance imaging (MRI) offers a realistic alternative to contrast-enhanced CT28 in the assessment of patients with acute pancreatitis. The avoidance of cumulative radiation exposure, potentially nephrotoxic iodinated contrast media, and the excellent contrast sensitivity and spatial resolution would make it an attractive alternative. Axial T1- and T2-weighted scans produce images analogous to those of CT. Gadolinium contrast enhancement can infer viability and improve anatomical definition. Heavily T2-weighted image acquisition, using a single breath hold and long repetition (TR) and echo (TE) times, results in little signal being produced by solid tissue, and a high signal from static fluid in the biliary and pancreatic ducts, enabling images anatomically comparable to those of ERCP to be produced. Whilst technically feasible in most centres, the MR environment is unsuitable for patients requiring significant circulatory or respiratory support, and at present few centres have the capability to perform MR-guided intervention. Contrast-enhanced CT therefore remains the imaging modality of choice for assessment and intervention in severe acute pancreatitis. However, MR has a role in the follow-up of acute inflammatory collections, where it is superior to CT in determining the extent of solid material within a collection (Fig. 13.3), and in excluding choledocholithiasis in selected patients. Management of acute pancreatitis in the UK is still based on two key guideline documents, now 726 and 1029 years old, respectively. The initial management of patients presenting with acute pancreatitis should be directed at the early identification and management of organ failure, most frequently renal and respiratory dysfunction. At present there are no established end-points of resuscitation to confirm that tissue perfusion and oxygen delivery have been restored adequately in patients with acute pancreatitis. Aggressive fluid resuscitation is often required, and monitoring the response to this relies upon traditional markers, in particular urine output, blood pressure and pulse oximetry. Physiological markers of resuscitation, for example acid–base balance from an arterial blood gas, may be helpful in detecting clinically occult hypoperfusion. Patients who do not respond to initial resuscitation, or who have evidence of organ dysfunction, should be transferred to a critical care environment for more invasive and intensive monitoring with central venous and arterial catheters. Respiratory failure should be treated with humidified oxygen, and this will be guided by continuous pulse oximetry and arterial blood gas analysis. Deteriorating respiratory function is a sign of disease progression. As many as half of all deaths from acute pancreatitis occur in less than 7 days, and the majority of these occur within 72 h of admission.1 There is evidence that patients managed in specialist institutions have a reduced risk of early death and this may be an indication that management of early MODS could be improved.
Acute pancreatitis
General description
Pathophysiology
Natural history
Diagnosis
Aetiology
Genetic defects
Iatrogenic causes
Inflammatory
Physiological
Assessment of severity
Single biochemical measures
C-reactive protein (CRP)
Other single predictive markers
Intra-abdominal hypertension (IAH)
Imaging

Role of CT
Role of magnetic resonance (MR)/magnetic resonance cholangiopancreatography (MRCP)
Management
Acute pancreatitis