Accessory Instruments for Operative Hysteroscopy
Rafael F. Valle
Michael S. Baggish
Various instruments for hysteroscopic surgery have been designed in flexible, rigid, and semirigid forms. The flexible and semirigid instruments range in size from 6- to 9-French (2 to 3 mm) and can be slid through the operating channel of the hysteroscope for intrauterine surgery. These include grasping forceps, biopsy forceps, scissors, and electrodes (Fig. 12.1). The rigid or fixed instruments cannot be slid into the hysteroscopic channel but must be attached to the sheath itself; therefore the attached telescope and sheath must negotiate the cervical canal as a unit. Very few surgeons use rigid instrumentation.
Most manufacturing companies offer at least two different types of instruments (Fig. 12.2A, B). Generally speaking, the smaller, flexible instruments are for light-duty procedures, since they are rather fragile. They do have the advantage of being positioned at varying angles by means of the deflecting sheath. Practically speaking, the need for this type of maneuver is infrequent. The larger, semirigid instruments are preferred if the given hysteroscopic sheath can accommodate the wider diameter (3 mm) of these devices. The 2-mm instruments are small enough to fit through standard operating channels (Fig. 12.3A, B). They may be manipulated for close-up work near the terminus of the telescope or slid out away from the telescope to permit panoramic surgery. Essentially, the location of the operating instrument is relatively independent of the optical portion of the hysteroscopic system (Fig. 12.4). The 3-mm instruments are manufactured to serve as heavier-duty equipment compared with the 2-mm semirigid devices. The flexible design of the larger instruments is resistant to bending and breakage. The stout-hooked scissors are well suited for rapid section of septa and are particularly useful for broad septum resection. The small scissors are practical only for thin septa and fine adhesions.
Although free intrauterine devices may be removed by either 2-mm or 3-mm forceps, the former are totally unsuited for imbedded devices. Only the larger biopsy instruments supply a satisfactory specimen for the pathologist to evaluate. The jaws of smaller instruments are simply too small to obtain an adequate specimen for interpretation. When Hyskon is used as the distending medium, all accessory instruments must be immediately and thoroughly washed with hot water. If the Hyskon dries on the jaws of these accessories and an attempt is made to force them open by working the handles, it is likely that the instruments will break. These instruments may be steam or gas autoclaved. The rigid instruments are classified as heavy instruments (Fig. 12.5). They are permanently incorporated into the construction of the specialized sheath. The telescope in effect looks through the interior of the rigid operating sheath (Fig. 12.6). Thus the optical system provides a limited field of view and is permanently tied to the operating instrumentation at a fixed, unalterable distance (Fig. 12.7). In fact, this distance is very close to the end of the telescope and produces a magnified close-up view with a small field. The size of these instruments permits cutting large lesions and clearly allows greater traction to be applied to intrauterine lesions. As noted, the instruments must be slid through the cervix as an operating system, with the instruments protruding beyond the sheath. This makes for a more traumatic and difficult entry into the uterine cavity. Additionally, the cervical canal is not viewed during entry.
Aspiration Devices
Plastic tubing may be required to clean up the uterine cavity (i.e., remove blood clots, mucus, and debris and/or wash the fluid when it has become mixed with blood). These catheters must be large enough to allow for this flushing effect and not become plugged with blood clots. The internal diameter of these catheters is 1.6 to 2.9 mm; the outer diameter, 2.0 to 3 mm (Fig. 12.8). Several types of plastic tubing have been roughly adapted for use as aspiration cannulae but usually suffer from being too short and not having the proper fittings for syringes to be attached. Some cannulae are banded with terminal 1-mm-spaced markings for purposes of measurement. These are available in lengths ranging from 35 cm to 100 cm and are constructed with Luer-lock fittings for easy leakproof syringe attachment. These aspiration cannulae are invaluable for suctioning debris out of the uterine cavity. Liquid media may be injected through the cannulae to flush the uterine cavity. Since they may be moved back
and forth, they are independent of the optical system. Most experienced hysteroscopists use aspiration cannulae freely and frequently. To attempt operative hysteroscopy maneuvers with less than optimal vision is fraught with unnecessary hazards. Simply aspirating debris transforms a cloudy field to one that is sharply clear and is well worth the modicum of time expended. The new large 3-mm cannula also may be adapted as a suction biopsy tool. New instrumentation couples injection and aspiration capability into a single device (Fig. 12.9).
and forth, they are independent of the optical system. Most experienced hysteroscopists use aspiration cannulae freely and frequently. To attempt operative hysteroscopy maneuvers with less than optimal vision is fraught with unnecessary hazards. Simply aspirating debris transforms a cloudy field to one that is sharply clear and is well worth the modicum of time expended. The new large 3-mm cannula also may be adapted as a suction biopsy tool. New instrumentation couples injection and aspiration capability into a single device (Fig. 12.9).
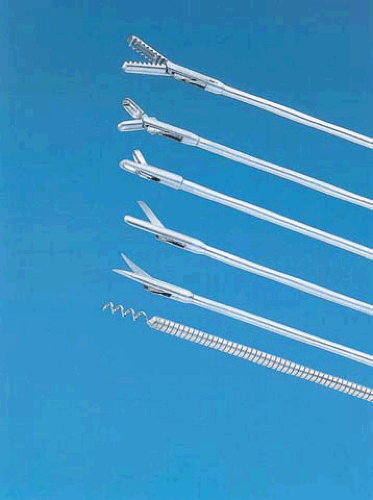 FIGURE 12.1 Various semirigid instruments that may be inserted through the operating channel of the hysteroscopic sheath include from TOP down: alligator grasping forceps, cup biopsy forceps, punch biopsy forceps, blunt end scissors, pointed scissors, myoma screw. |
Electrodes
Several types of electrodes may be inserted through operative sheaths. With the recent development of the large (3 mm) operative channel sheath, a new crop of specialized electrodes including both monopolar and bipolar types have been produced. These electrodes can do everything that the resectoscope is capable of doing and more. Among the monopolar electrodes are a 2.5-mm ball electrode, a 2.5-mm button electrode, a needle electrode, and a retractable loop electrode (Fig. 12.10A–C). The 3-mm isolated channel allows for the use of the only bipolar technology for operative hysteroscopy in the form of bipolar hysteroscopic needs, bipolar ball. Bipolar hysteroscopy devices are currently available in a wide variety of configurations including bipolar resectoscopes (Fig. 12.11A, B).
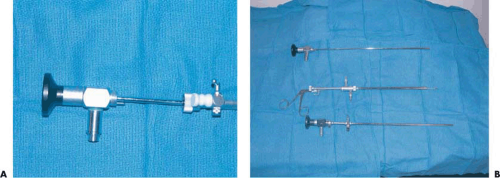 FIGURE 12.2 A: The telescope is partially withdrawn from the operative sheath. A rubber gasket has been affixed to the entry port of the operating sheath. The stopcock for the sheath is in the closed portion. B: A semirigid hysteroscopic scissors has been fully inserted into the operating channel. Note the channel’s stopcock is now in the full opened position. |
Operating Plugs
Most operating sheaths are equipped with a single access channel. The operating channel is fitted with a stopcock that can be switched to an open or closed position to prevent leakage of the distending medium. When a flexible instrument, electrode, semirigid instrument, laser fiber, or aspiration cannula is engaged into the channel, a gasket or nipple must be applied to the fitting of the channel to suppress leakage. Until recently, adaptations of urologic rubber nipples have been used (Fig. 12.12A). Some of these nipples
have oversized openings, which results in leakage of media when narrow-gauge instruments are inserted. Those nipples with pinpoint openings are best suited for operative hysteroscopy (Fig. 12.12B).
have oversized openings, which results in leakage of media when narrow-gauge instruments are inserted. Those nipples with pinpoint openings are best suited for operative hysteroscopy (Fig. 12.12B).
 FIGURE 12.3 A: Close-up view of semirigid alligator forceps. B: Close-up view of semirigid straight scissors. |
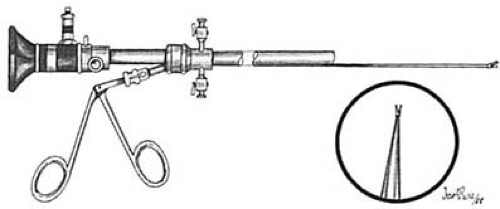 FIGURE 12.4 View through telescope using semirigid scissors. |
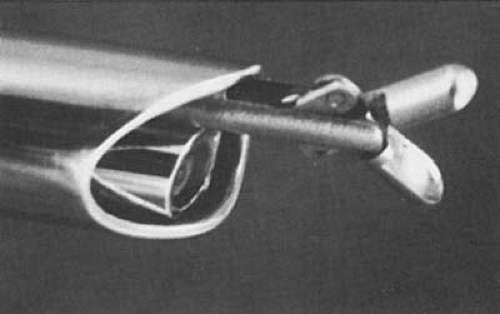 FIGURE 12.5 The rigid forceps is fixed and protrudes slightly beyond the specialized sheath. |
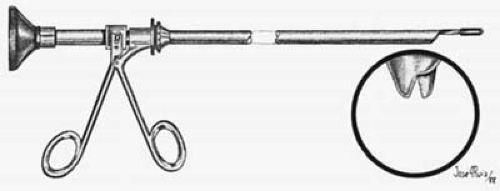 FIGURE 12.6 View through rigid scissor sheath. |
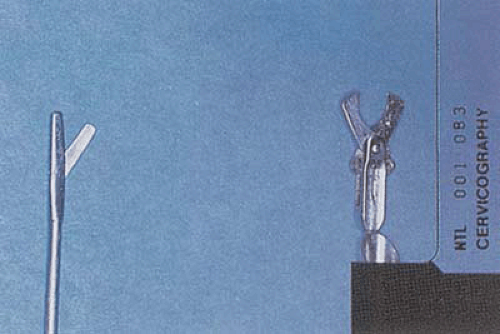 FIGURE 12.7 Close-up comparison between semirigid and heavier rigid scissors. |
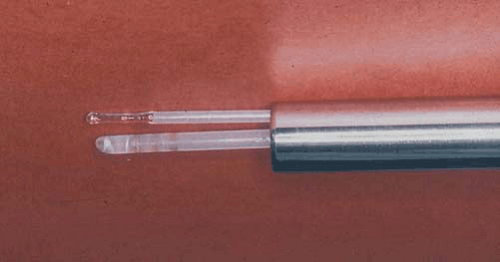 FIGURE 12.8 Dual-channel hysteroscope with 600-micron laser fiber inserted through one channel and an aspirating cannula through the second channel. |
An alternative operating gasket that attaches to the sheath channel by means of a Luer-lock connection has appeared on the market. This plug design precludes slippage. Additionally, the fine-leaf construction of the gasket provides very close clearance for the narrow-gauge laser fibers and thereby reduces leakage of media with even extreme side traction.
Extension Cannulae
Hyskon can be injected into the operating sheath by attaching a 60-mL syringe directly to the Luer-lock fitting of the medium instillation port of the hysteroscopic sheath. This method has several drawbacks. First, the angle for injection is awkward and does not allow adequate pressure to be applied, especially when the diagnostic sheath is used. Second, attachment and detachment of syringes are awkward. Third, not infrequently the syringe angulates to the side and becomes detached; the operator is then sprayed with Hyskon. It is more advantageous and convenient to inject Hyskon by the incorporation of an intermediary, large-diameter connecting tube (Fig. 12.13A, B). This should be approximately 12 cm long with a 4-mm outer diameter. This tube must be constructed with Luer-lock fittings to couple securely to the hysteroscope sheath and to allow very secure attachment of the 60-mL injection syringe. Additionally, these extension tubes are convenient for nonviscid liquid media (e.g., saline, glycine, mannitol instillation).
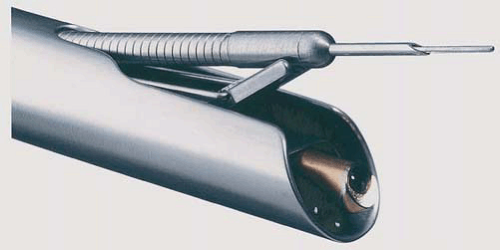 FIGURE 12.9 An injection aspiration device exits the operating channel and may be directed via a terminal bridge, which is part of this operative sheath. |
Hysteroscopic Cart
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


