It is necessary hoe hym that is sycke to have two or three good keepers.
—ANDREW BOORDE (1490-1549): The Dyetary of Helth XL
The care of the patient who will undergo or who has undergone ostomy surgery involves close cooperation among the surgeon; the wound/ostomy, continence (WOC) nurse; and the patient in order to achieve optimal rehabilitation. Parenthetically, the nursing specialty of “enterostomal therapy” has been replaced by the title, “wound, ostomy, and continence nursing.” As discussed in Chapter 31, the technique for fashioning an ostomy falls within the purview of the surgeon. However, much of the physical, emotional, and educational aspects of the rehabilitation process usually fall within the domain of the WOC nurse.6,14 Still, if a WOC nurse is not available, responsibility for stoma assessment, fitting, and rehabilitation still properly rests with the surgeon.6
▶ PREOPERATIVE CARE
As stated in Chapter 31, optimal postoperative stomal management begins with preoperative preparation.8 The patient and family members ideally should receive comprehensive information concerning overall ostomy rehabilitation, plans, and management. This includes activity, diet, clothing, and sexual concerns. The patient should be reassured that selfcare may, at first, seem awkward, but all can be mastered by almost any patient at any age in a relatively short time.8 Contact with an ostomy visitor may be especially beneficial. A confident, fully rehabilitated ostomy/site visitor can provide hope and improve morale for the apprehensive patient.
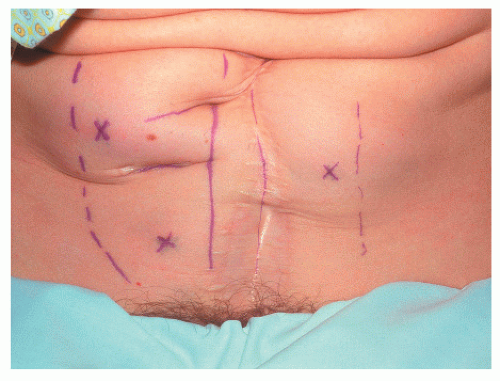
As discussed in Chapter 31, the site should ideally fall below the umbilicus in the left or right lower quadrant, on the superior aspect of the infraumbilical fat mound, and should lie within the surface marking of the rectus sheath (see Figures 29-39 and 29-40).7,14 It is important to avoid scars, creases, and bony prominences in order to provide a smooth pouching surface postoperatively (Figure 32-1). It is also imperative for the individual to see the site. To accomplish this, the patient is evaluated while he or she is supine, sitting, and standing because positional changes can materially alter the abdominal configuration (Figure 32-2). A patient with a protuberant abdomen or someone requiring long-term use of a wheelchair may be better served with a stoma located in the upper abdomen.7 It is axiomatic that self-care will be rendered difficult or impossible if the patient is unable to see the stoma. Although stoma site selection is truly the responsibility of the surgeon, it is appropriate and reasonable to delegate this task to a WOC nurse.14 Preoperatively, using a surgical marking pen or a fine-gauge needle (see Figure 29-40) provides a guide to the ideal location so that intraoperative guessing is eliminated. Even those patients who undergo emergency or temporary stomas should optimally have preoperative stomal marking.7,14
Independence in ostomy care requires integration of the stoma into the patient’s everyday life. In addition to site selection, stoma construction itself can have a profound influence on the effectiveness of a pouching system (see Chapters 29 and 31). A budded stoma in a preselected location offers the best chance for successful ostomy management. A patient who is offered a comprehensive preoperative educational program is much more likely to be an active participant in postoperative activities. Even those individuals in whom there is only the possibility of a stoma or in whom the stoma is to be temporary should be marked and offered counseling preoperatively by the surgeon and/or the WOC nurse.8 National guidelines for enterostomal patient education have been established by the Standards Development Committee of the United Ostomy Association, with the assistance of Prospect Associates.2
FIGURE 32-1. Selection of potential stomal sites is particularly difficult in this obese patient with a left paramedian incision. Note the deep scar from a prior stoma in the right lower quadrant. The dashed lines represent the outer border of the rectus muscles. The optimal site for this individual is the one marked on the left side.
FIGURE 32-2. Site selection was inappropriately marked on both sides with the patient supine. The X‘s in the superior aspect were elected because the inferior ones would have fallen below the fat bulge.
▶ STOMAL FUNCTION AND CARE
Fecal and urinary diversion may be performed in patients for a variety of clinical indications and situations. A brief overview of these various stomas follows.
Gastrointestinal Stomas
Jejunostomy
Jejunostomy function usually begins within the first 48 hours after surgery. If the stoma was created laparoscopically, function will usually commence earlier. Initially, the effluent is watery, clear, and dark green. Because the volume of output may approach 2,400 mL in 24 hours, the patient must be monitored closely for electrolyte imbalance. Because the absorption of nutrients, fluids, and electrolytes may be deficient in a patient with a jejunostomy, total parenteral nutrition or fluid/electrolyte support may be required.14 In order to minimize the inconvenience associated with the need for frequent pouch emptying, connection to gravity drainage is advisable.
Ileostomy
An ileostomy generally begins to function within the first 48 to 72 hours after surgery, although those undergoing laparoscopic construction may evidence an effluent within 24 hours. The initial appearance may be viscous and green, but such an output does not necessarily indicate the return of peristalsis. Rather, it may represent the elimination of secretions that have collected in the distal small bowel. Once peristalsis has returned, the patient may enter a period of high-volume output known as the adaptation phase. Output during this time may exceed 1,000 mL/day, frequently reaching 1,500 to 1,800 mL/day. The physiologic basis for this high-output phase is the loss of the colonic absorptive surface, coupled, theoretically, with the loss of the ileocecal valve. During this period, the patient should be monitored for signs and symptoms of fluid and electrolyte imbalance.
A loop ileostomy-supporting rod is removed by the third to fifth postoperative day, depending on the amount of edema of the stoma itself. The greater the swelling, the earlier the rod may be removed. The less tissue reaction present, the longer the rod should be maintained. Edema itself tends to prevent the stoma from retracting, and the rod may actually intensify and prolong the duration of the edematous reaction. Patients with a loop ileostomy proximal to a pelvic pouch will experience a higher output and have an increased risk for fluid and electrolyte management problems. Readmission may be necessary for these individuals, and early stomal closure may be required for this indication. As with jejunostomy, connection of the pouch to gravity drainage will prevent overdistension of the appliance. If the stool thickens but output remains high, use of anesthesia tubing and a plastic bottle can be adapted. This is especially convenient if one uses a two-piece pouching system. While ambulating, the patient can wear a standard pouch and closure clamp, but a second pouch secured to the gravity drainage system can be attached while one is resting.
Over a period of days to weeks, the proximal small bowel increases fluid absorption. Gradually, the volume of output decreases and the stool thickens to toothpaste-like consistency. Initially, the output from an ileostomy can vary from 500 to 1,500 mL in a 24-hour period. But, after adaptation, the average output decreases to between 500 and 800 mL/day.14
Continent Ileostomy
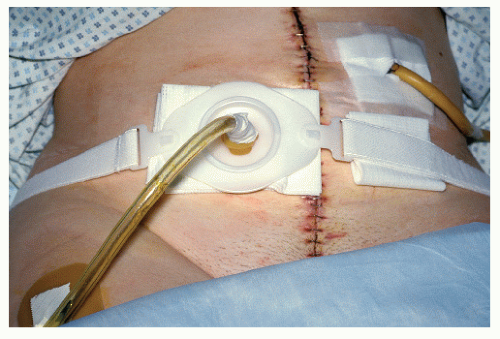
Since the advent of the pelvic pouch procedure (see Chapter 29), the continent ileostomy today is primarily performed for the indications of an elective conversion in those with a permanent, conventional (Brooke) ileostomy; for those with a failed reservoir-anal procedure; and for patients with anal incontinence. One of the important concerns is to stabilize the defunctioning drainage catheter that is placed in the pouch (see Figures 29-70 and 29-72). This may be achieved through a variety of methods, including a stomal plate, ostomy appliance belt, or a baby nipple (Figure 32-3). A sterile gauze dressing around the stoma will absorb mucous and moisture as well as afford protection.9,18
FIGURE 32-3. Continent ileostomy stoma plate. Baby bottle nipple anchors catheter device after removal of tripod sutures.
To minimize tube blockage, gentle irrigation with 20 to 30 mL of normal saline is recommended, commencing in the recovery unit and continuing every 2 to 3 hours for the next few days.9,18 Intervals between irrigations can be increased based on how well the tube is draining. It is extremely important to avoid overdistension of the pouch for the first few weeks following surgery in order to limit the likelihood of desussception. A bedside drainage bag or leg bag must be used to maintain constant drainage.
Colostomy
The initial output from a colostomy varies depending on the location of the stoma within the colon. Because the colon absorbs all but approximately 100 mL of the 1,000 mL of contents that passes through the ileocecal valve daily, the output from distal colonic stomas has a thicker consistency and smaller volume than that of proximal colonic stomas.
Cecostomy
A cecostomy usually begins to function by the third postoperative day. The output may be projectile (because of close proximity to the ileocecal valve), and it is initially liquid. The place of cecostomy in colon and rectal surgery has been discussed in the previous chapter and in Chapter 20. A cecostomy may be either skin level or tubal (see Figures 28-59 and 31-45). As has already been discussed in this text, the location, output characteristics, and construction combine to make this a difficult stoma with which to deal. The tube cecostomy poses a special management problem because stool tends to flow both through and around the tube. Furthermore, tube cecostomies are also associated with a greater risk of intra-abdominal spillage.
Transverse Colostomy
A transverse colostomy usually begins to function on postoperative day 3 or 4. Output, which varies from pasty to soft, usually occurs after meals and at intervals throughout the day. For a loop colostomy, a supporting device (e.g., rod or bridge) placed during surgery is removed 3 to 5 days later (see Chapter 31). Corman and Odenheimer have described numerous methods for creating a loop colostomy in order to maintain stomal support.5
Descending/Sigmoid Colostomy
A descending or sigmoid colostomy requires the longest time to regain normal function, perhaps not until postoperative day 5. After this period, one logically should be concerned with issues that may cause delay in colonic function—ileus, administration of narcotics, obstruction, and so on. One may consider the option of stimulating colonic evacuation by means of a no. 20 French Foley catheter gently advanced into the stoma. A warmed solution of 500 mL of normal saline can be instilled via gravity drainage and allowed to return.6,8,14 This procedure initiates a reflex contraction, stimulating peristalsis and providing relief of gaseous distention. Because many patients with a colostomy are discharged as early as the fourth postoperative day, self-care instruction may not be adequate because of the lack of output. Another alternative is to use a stool substitute placed in the pouch to assist in teaching pouch-emptying techniques. Instruction is continued following hospital discharge in the patient’s home or in the outpatient department.
Once normal bowel function has returned, the output from a descending or sigmoid colostomy usually is a soft, formed stool. Elimination patterns generally are the same as that experienced by the patient before he or she became ill. Colostomy irrigation with a cone may also be performed as a management option to avoid an appliance in selected patients or in preparation for diagnostic testing (Figure 31-25). The technique for colostomy irrigation has been discussed in Chapter 31. However, instructions for the patient appear here in Tables 32-1 and 32-2.
Urinary Stomas
Vesicostomy
Drainage is provided by a Foley catheter placed in the anterior dome of the bladder. Should pouching be requested, the suprapubic location may make obtaining a secure seal problematic. Shaving the pubic hair is helpful in order to facilitate pouch adherence and removal.
Ureterostomy
Creation of unilateral or bilateral ureteral openings to the skin is uncommonly employed. The flush or retracted stoma associated with ureterostomies can pose a real pouching challenge. If the stoma is located in the flank, self-care may be impossible. Therefore, a family member or other home caregiver should be instructed on how to manage this ostomy.8
Nephrostomy
Generally, nephrostomies are managed by means of a sterile closed drainage system. A skin barrier wafer is usually placed on the skin around the tube to protect the skin and to anchor the tube to prevent accidental dislodgement.8
TABLE 32-1 Colostomy Irrigation with a Cone
1.
Apply the irrigation sleeve securely around the stoma to prevent leakage.
2.
Close the shutoff valve. Fill the irrigation bag with 500-100 mL of tepid water and hang the irrigation bag on a hook.
3.
Remove air from the tubing by opening the shutoff valve until the water runs out of the cone. Close the shutoff valve and lubricate the end of the cone with water-soluble lubricant.
4.
Sit up straight on a chair or toilet with irrigating sleeve just touching the water level in the toilet bowl.
5.
Open the shutoff valve until the water flows slowly. Insert the lubricated cone into the stoma until the water enters without leakage. Increase the flow rate as tolerated. If a cramp develops, stop or decrease the water flow until the cramp passes and then resume the water flow.
6.
When the 500-1,000 mL of water has entered the colon, remove the cone and close the top of the irrigation sleeve. The bottom of the irrigation sleeve should remain in the toilet bowl for no less than 15 minutes. By then, the majority of the stool and water will have returned.
7.
Rinse the inside of the irrigation sleeve with water to remove the waste material. Remove the irrigation sleeve from the bowl. Dry and clip the bottom of the irrigation sleeve to the top of the sleeve. It may take up to 45 minutes for the rest of the water and stool to return.
TABLE 32-2 Colostomy Irrigation Helpful Hints
Spray the inside of the irrigation sleeve with any liquid soap or detergent prior to administering the enema so that the stool will drain easily, the sleeve will clean faster, and less odor will be retained.
During the enema, if you experience
CRAMPING:
May indicate constipation; recall firmness of prior evacuation.
Slow or stop the flow of water, relax and deep breathe.
Recheck the rate of water flow; flow rate should be approximately 10 minutes for 1,000 mL of water; 5-7 minutes for 500 mL.
Check the height of enema bag; it should be approximately 12-20 in. (30-50 cm) above the shoulder level when one is seated.
SLUGGISH/NO RETURNS:
May indicate constipation; recall firmness of prior evacuation.
Look at diet; may need to increase bulk, such as bran, fresh fruits, and vegetables.
May indicate dehydration; increase oral fluid intake to 8 glasses of liquid per day.
Increase physical activity.
After the enema, if one experiences
SPILLAGE:
May indicate constipation; recall firmness of prior evacuation.
Look at the volume of water inserted during the enema; most individuals require 1,000 mL.
Do not use more than 1,000 mL without physician’s permission.
Check that the enema solution does not escape around the cone or shield.
EXCESSIVE GAS OR FLATUS:
Avoid gas-forming foods.
Eat regular meals; chew food well.
Avoid air swallowing, that is, mouth breathing, gum chewing, smoking, straws, carbonated beverages, alcohol.
Conduits
Ileal, jejunal, and colonic conduits are frequently employed methods for effecting urinary diversion. Preoperative stoma sighting and construction of a properly budded stoma will improve the potential for obtaining a secure pouch seal.
Continent Urinary Diversion
A variety of forms of continent urinary diversion are performed. Preoperative and postoperative management techniques for these types of diversion are similar to that of continent ileostomy.
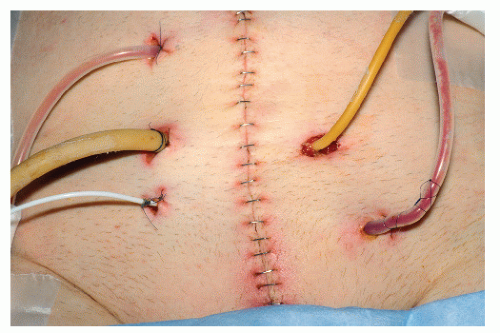
The ileocecal reservoir, commonly known as an Indiana pouch, uses a variety of tubes and drains. Drainage of the newly created urinary reservoir is accomplished by means of a cecostomy tube, bilateral urinary stents, and a catheter placed into the plicated exit conduit (Figure 32-4).1,9,18 Depending on the surgeon’s preference, gentle irrigation of the cecostomy tube with 20 to 30 mL of normal saline is performed every 2 to 3 hours.9 As with the continent ileostomy, the goal is to maintain the patency of the catheter and to prevent overdistension of the newly created reservoir. It is not uncommon to cap the catheter into the exit conduit to avoid disruption of the newly plicated ileal segment.
FIGURE 32-4. Multiple drains including ostomy tube in a patient who underwent a continent urostomy (ileocecal reservoir), a so-called Indiana pouch.
Stabilization of the tubes and drains can be achieved by a variety of tube anchoring devices. Use of constant drainage by means of a bedside drainage bag or leg bag is recommended for the first few weeks after surgery.9,18
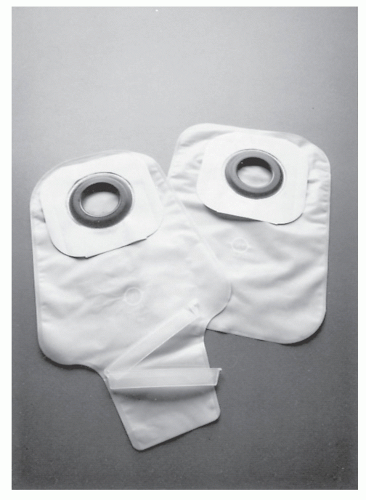
FIGURE 32-5. Drainable and closed pouches with karaya seal and adhesive. (Courtesy of Hollister, Inc.)
▶ OSTOMY MANAGEMENT
Immediate Postoperative Period
Proper application of a pouching system should begin in the operating room. The appliance is fixed to clean, dry skin in order to protect the incision and the peristomal skin and to contain stomal discharge. Although it is true that most fecal stomas will not begin to function for a few days, mucosal secretions are ideally collected with a pouch. Conversely, urinary stomas will function immediately unless anastomotic disruption of the urinary-bowel connection has occurred. Pouch application coupled with connection to gravity drainage is indicated for urinary stomas.
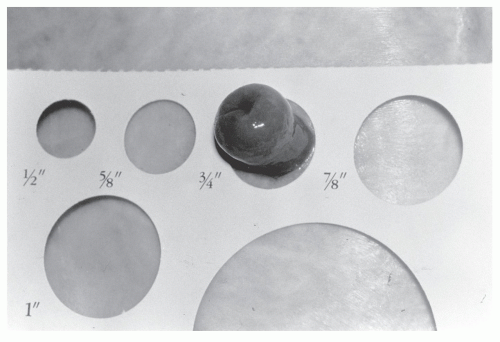
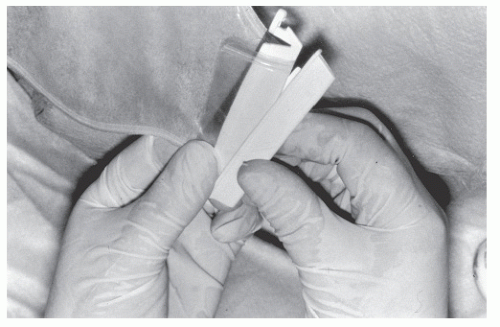
A variety of one-piece or two-piece, disposable, odorproof, pouching systems may be used (Figure 32-5 and Table 32-3). By using a disposable measuring guide and by sizing the aperture of the pouch within 1/8 in. (3 mm) of the base of the stomal mucosa, one can protect the peristomal skin and prevent mucosal trauma (Figure 32-6). Removal of the release paper and gentle pressure on the abdomen following pouch application will enhance pouch adherence. A transparent, drainable pouch will permit the clinician to assess stoma viability as well as output. A closure clamp or tubing device is then securely applied (Figure 32-7).
A healthy, viable stoma appears moist, beefy red, and often edematous. However, a continent ileostomy stoma may have a darker, bruised appearance due to mesenteric venous compression. Some individuals with a history of using senna-containing laxatives may demonstrate melanosis coli in the mucosa of their colostomy. This stoma may appear moist and gray to brown or even black in appearance due to staining of the bowel mucosa (see Figure 20-1 A).
TABLE 32-3 Pouching Systems
TYPE
FEATURES/VARIETIES
One-piece drainable, closed-end urostomy
Flexible, semiflexible, firm, with or without skin barrier attached. Flat and with convexity ranging from shallow to very deep precut and cut to fit.
Two-piece
With or without adhesive tape collar.
Precut and cut-to-fit varieties.
Built-in convexity or option of convex insert.
Adult/pediatric sizes.
Pouch removable without disturbing flange.
Clear and opaque pouches.
Variety of size and shapes of pouches, irrigation sleeves, and stoma caps.
Belt hooks for optional belt use. Provides sense of security especially for very active ostomates.
Pouching tips
Peel off all backing paper.
Size properly—decrease aperture as stoma edema decreases.
Assess need for convexity.
Close pouch properly.
Be alert for candidiasis.
Snap on pouch securely to flange in two-piece system.
FIGURE 32-6. Disposable measuring guide permits use of properly sized faceplate.
Assessment of the mucosa is evaluated with each pouch change. Viability and function can be evaluated daily by the surgeon, by the WOC nurse, and by each shift of the nursing staff.
Principles of Fitting
In order to provide some appreciation for the alternative methods of managing ostomies, it is important to have an understanding of ostomy collection devices. It is not important for a surgeon to be familiar with every company and every product in the field. It is merely necessary to be aware of the general principles for using the various devices and to have, perhaps, one or two alternatives from which to choose should the need arise.
Three primary parts—skin barrier, faceplate, and pouch— are necessary for an effective collecting system, but there are a variety of additional accessories.11 The newer generation of appliances incorporates these parts into a single disposable or reusable system.
FIGURE 32-7. Applying closure clamp to drainable pouch.
Skin Protective Agent
A skin sealant, such as Skin Prep (Smith and Nephew), provides a clear film that coats the skin. Generally, protective agents are used when tapelike products (e.g., double-faced disks) or cement contact the skin in order to limit the likelihood of irritation. They also augment adherence of an appliance and facilitate adhesive removal from reusable faceplates.19 These protective agents are available as gels, sprays, wipes, paint-on solutions, or pastes. Distinction must be made between a skin barrier and a protecting agent; individuals with ileostomies should never use a protective agent in place of a skin barrier.
Skin Barrier
A skin barrier is an adherent porous material that offers protection from the contents of the colon or ileum (e.g., karaya or carboxymethylcellulose-based products). Preserving the integrity of the skin is of great concern in the immediate postoperative period. Moist, weeping, oily, eroded skin will lead to leakage, odor, and loss of appliance adhesion. Meticulous attention to skin care must begin in the operating or recovery rooms with the first application of the skin barrier and placement of the pouch. The most commonly employed skin barriers are discussed in the following sections.
Karaya Products
Karaya is a resin that forms a protective base when combined with glycerin, thus inhibiting the corrosive effects of ileal contents. It is relatively insoluble and quite hydroscopic. It is refined and marketed in different forms, including powders, washers, wafers, and blankets, and mixed with natural clays. It is also manufactured in paste form, which provides an excellent means for filling in crevices created by abdominal folds near the stoma. Karaya stretches, and when it is used as a washer, it should measure about 1/4 in. smaller than the base of the stoma in order to fit it snugly. Specially prepared hole-cutter tools are available from several ostomy manufacturers (Figure 32-8).
Karaya is nonallergenic, although the ingredients in some products may cause some sensitivity. If this is a problem, a change to a karaya product manufactured by another company may be all that is required.
FIGURE 32-8. Hole cutter tool. A steel blade is mounted in a plastic handle. This can be prepared by request for various diameters. (Courtesy of Nu-Hope Laboratories.)
One disadvantage of karaya products is the tendency to break down in the presence of urine. Therefore, they should never be used with urinary diversions. Karaya melts easily in heat or even when the patient has an elevated temperature. Thus, for ostomates who live in warm climates, a different skin barrier should be used (e.g., Stomahesive or Hollihesive). Generally, the use of karaya is advised less often than the products subsequently discussed.
Only gold members can continue reading. Log In or Register to continue