CHAPTER 1 Uroradiology
![]() What are the specific radiological findings depicted below and what diagnosis do they suggest?
What are the specific radiological findings depicted below and what diagnosis do they suggest?
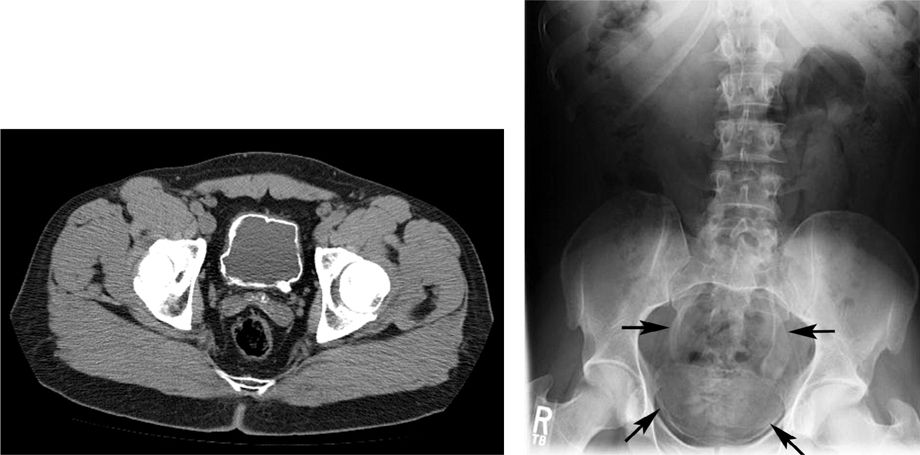
Diffuse bladder wall and distal ureteral calcifications suggest schistosomiasis of the bladder and ureters. Nodular bladder wall thickening occurs in the acute phase, which is followed by bladder wall fibrosis and calcification. Calcification of the ureter and seminal vesicle may also occur. This diagnosis should be suspected when a patient gives a history of travel to an endemic region (the Middle East, India, Africa, and Central and South America) and presents with frequency, urgency, hematuria, and dysuria. Abnormal appearance of the bladder is secondary to deposition of eggs, which subsequently calcify, into the bladder wall from the pelvic venous plexus. Squamous cell carcinoma can be a long-term complication. The computed tomography (CT) axial image on the left demonstrates circumferential bladder wall thickening and calcification extending into the left ureter in a patient with schistosomiasis. Abdominal x-ray in a similar patient, a 27-year-old refugee from Africa, also demonstrates diffuse bladder wall and bilateral ureteral calcifications. Diagnosis is confirmed by a blood test for parasitic antigens or by finding eggs in the urine or stool. Treatment is with a single dose of praziquantel. A total of 240 million people worldwide are affected by this parasite, which uses a snail as an intermediate host.
![]() A 23-year-old man has a history of microscopic hematuria and an intravenous urogram (IVU) is planned for evaluation. The patient reports a history of an allergy to shellfish. He has not previously received IV contrast. The next step should be?
A 23-year-old man has a history of microscopic hematuria and an intravenous urogram (IVU) is planned for evaluation. The patient reports a history of an allergy to shellfish. He has not previously received IV contrast. The next step should be?
Patients with a history of asthma, drug allergy, or allergy to shellfish have approximately a 2-fold greater risk of a contrast reaction. Minor reactions include hot flushes, nausea, vomiting, or urticaria while major reactions include bronchospasm, hypotension, laryngeal edema, and cardiac arrest. The overall incidence of contrast reactions is estimated to be 13% with high-osmolality agents and only 3% with low-osmolality agents. The alternatives to consider in this patient include substitution of a different study (particularly had there been a severe prior reaction), the use of lower osmolality contrast agents, and pretreatment with steroids and antihistamines. A reasonable pretreatment regimen for adults consists of 50-mg prednisone at 13, 7, and 1 hour prior to the study, and 50 mg of diphenhydramine 1 hour before the examination. H1 and H2 blockers can also be used.
Another option would be to use either ultrasound and/or noncontrasted CT scan to examine the kidneys in a case of microscopic hematuria, particularly when the patient is only 23 years old.
Contraindications to IVP include previous anaphylactic reactions to IV contrast and positive azotemia (creatinine >2.0). Relative contraindications include dehydration, diabetes, multiple myeloma, and pregnancy.
![]() A 30-year-old female is undergoing a workup for microhematuria. Her serum pregnancy test is negative. The 15-minute film from the IVU is shown. The next step should be?
A 30-year-old female is undergoing a workup for microhematuria. Her serum pregnancy test is negative. The 15-minute film from the IVU is shown. The next step should be?

The patient should have a cystoscopy to complete the workup. The IVU is normal. (It is not uncommon to have a normal study appear on a board examination.) While the film as shown is normal, it is important to point out that the top of the left kidney is “cropped.” The entire kidney should be visible on an IVU. If not, additional films should be taken.
![]() Describe the proper technique for performing and reviewing an IVU.
Describe the proper technique for performing and reviewing an IVU.
In a normal IVU, a kidneys, ureters, bladder (KUB) or scout film is obtained following which approximately 1 cm3/kg of IV contrast is administered. On the KUB, careful attention should be paid to any and all unusual calcifications, organs outside the urinary tract, and bony abnormalities as well as any technical flaws. A 30-second film shows the nephrogram phase of the IVU and is regarded as the best film to assess renal masses and renal contour. During the excretion phase, 5-, 10-, and 15-minute films are generally taken. There should be symmetric excretion. The left kidney should be no more than 2-cm longer than the right kidney. Kidneys should be approximately 3 to 5 vertebral bodies in length. Forniceal angles should be sharp. Blunting of the forniceal angles is said to be the earliest radiographic sign of hydronephrosis on IVU. Three major infundibula should be visualized along with roughly 13 to 14 calyces for each kidney. The angle, orientation, outlines, shape, and position of the kidneys should be reviewed and tomograms should be taken if there is any doubt about the integrity of the kidneys. The ureter should not show a standing column (columnization) of contrast and the bladder contour, best seen on the 15-minute film, should be smooth. A postvoid film should also be done. Posterior oblique films can be performed to better visualize the distal ureters.
![]() A 70-year-old man presents with microhematuria and a portion of the initial KUB done for the IVU is shown. Prior to cystoscopy, what should be the next step?
A 70-year-old man presents with microhematuria and a portion of the initial KUB done for the IVU is shown. Prior to cystoscopy, what should be the next step?
Four things to look for on the scout film are “masses, gasses, bones, and stones.” Each time you look at a scout film review those 4 things and comment about whether they are normal or abnormal. Symmetry is also important. In this case, there is asymmetry on either side of the pubic symphysis with sclerosis evident on the left. There is a somewhat moth-eaten appearance to the periosteum on the left superior and inferior pubic rami as well. Sclerotic bone lesions are found in patients with breast and prostate cancer. On plain films, a 50% change in cortical density is required to visualize metastatic disease. In this elderly man, the next step should be a prostate-specific antigen and a prostate examination.
![]() A child with multiple birth defects had a renal ultrasound suggestive of duplication and hydronephrosis. An IVU was performed to further evaluate the finding. The KUB obtained prior to the study is shown. What is the radiographic finding demonstrated?
A child with multiple birth defects had a renal ultrasound suggestive of duplication and hydronephrosis. An IVU was performed to further evaluate the finding. The KUB obtained prior to the study is shown. What is the radiographic finding demonstrated?
The radiograph is a classic picture of complete sacral agenesis. The sacrum is absent causing the pelvic ring to look like an inverted teardrop. Incomplete agenesis may be more difficult to diagnose. The diagnosis may be delayed until failed attempts at toilet training prompt urological evaluation for neurogenic bladder. Sacral agenesis may be one component of the VACTERL syndrome (V = Vertebral anomalies, A = imperforate Anus, C = Cardiac anomalies, TE = Tracheoesophageal fistula, R = Renal anomalies, and L = Limb anomalies).
![]() This KUB accompanied the IVU done for evaluation of congenital urological problems in a child. What is the radiographic finding demonstrated?
This KUB accompanied the IVU done for evaluation of congenital urological problems in a child. What is the radiographic finding demonstrated?
The 3 conditions that are associated with widening of the symphysis pubis include pregnancy, trauma, and the congenital condition of exstrophy/epispadias, of which this is an example. The femurs are rotated laterally. There is no separation of the sacroiliac (SI) joint to suggest trauma. This abnormality is thought to occur as a result of failed mesodermal ingrowth and consequent failure of descent of the cloacal membrane that produces eventration of the bladder onto the abdominal wall. The spectrum ranges from pure epispadias with a dorsal penile meatus and urethra to cloacal exstrophy with eventration of both bowel and bladder.
![]() A 35-year-old female presents many years after a sterility procedure in which silicone was injected into the fallopian tubes. She has had significant microscopic hematuria. The likely diagnosis is?
A 35-year-old female presents many years after a sterility procedure in which silicone was injected into the fallopian tubes. She has had significant microscopic hematuria. The likely diagnosis is?

The diagnosis is a bladder stone secondary to foreign body, which in this case was the silicone that eroded through the bladder wall producing a nidus for stone formation. It is important to consider the possibility of outlet obstruction or foreign body when treating a patient with a bladder stone.
![]() This plain film was obtained in a patient undergoing a workup for microhematuria and pyuria. A routine urine specimen submitted for culture was negative. What is the likely diagnosis?
This plain film was obtained in a patient undergoing a workup for microhematuria and pyuria. A routine urine specimen submitted for culture was negative. What is the likely diagnosis?
This film shows the classic “paste” stones of genitourinary tuberculosis. The stones are faint on plain film and represent dystrophic calcification of the caseating granulomas that infiltrate the parenchyma of the kidney. The tissue sloughs into the collecting system giving rise to these stones.
![]() A 20-year-old diabetic female presents to the emergency department with fever to 104°C and a white count of 33,000 associated with a left shift. The scout film from an IVU is shown. What is the most likely diagnosis?
A 20-year-old diabetic female presents to the emergency department with fever to 104°C and a white count of 33,000 associated with a left shift. The scout film from an IVU is shown. What is the most likely diagnosis?

There is gas 0essentially replacing the left renal outline in a classic case of emphysematous pyelonephritis. The treatment is broad-spectrum antibiotics and nephrectomy. A CT scan, if the patient is stable enough to tolerate the procedure, may help to distinguish a perinephric abscess caused by a gas-forming organism. Gas may outline the kidney in cases of duodenal or colon (retroperitoneal) trauma as well.
![]() An elderly man presents with obstructive voiding symptoms, microhematuria, and a palpable abdominal mass. A KUB was obtained prior to the IVU. The next step should be?
An elderly man presents with obstructive voiding symptoms, microhematuria, and a palpable abdominal mass. A KUB was obtained prior to the IVU. The next step should be?
The plain film while overpenetrated shows a midline abdominal mass extending from the pelvis to well above the presumed umbilicus. The next step should be to place a Foley catheter, which in this case resulted in resolution of the mass. This is a bad case of urinary retention.
![]() A patient undergoing a workup for microhematuria has the following KUB obtained prior to the IVU. What is the radiologic finding and what are the top 3 possible diagnoses associated with this radiographic finding?
A patient undergoing a workup for microhematuria has the following KUB obtained prior to the IVU. What is the radiologic finding and what are the top 3 possible diagnoses associated with this radiographic finding?
The film shows medullary nephrocalcinosis. This finding is seen most commonly with medullary sponge kidney, type 1 renal tubular acidosis, and hyperparathyroidism. Cortical nephrocalcinosis is rarely seen in the present era. In the past, it typically was seen as a consequence of postpartum hypotension and renal infarction that produced atrophic kidneys with calcified cortices.
![]() This scout film was obtained to evaluate left flank pain and fever. The urinalysis shows a pH of >7.2 and many gram-negative rods. What are the significant findings on the film? What is the most likely organism cultured from the urine? In addition to antibiotics, what immediate procedure is probably necessary?
This scout film was obtained to evaluate left flank pain and fever. The urinalysis shows a pH of >7.2 and many gram-negative rods. What are the significant findings on the film? What is the most likely organism cultured from the urine? In addition to antibiotics, what immediate procedure is probably necessary?

This film shows a large staghorn calculus on the right and multiple stones in both the kidneys. To be classified as a staghorn calculus, the stone should fill and outline at least one calyx and infundibulum. In addition, there appears to be a large calcification medial to the left kidney, which could represent ureterolithiasis. These are likely magnesium ammonium phosphate (struvite or triple phosphate) stones associated with urea splitting organisms such as a proteus species accounting for the alkaline urinary pH. Subsequent films confirmed obstruction on the left and a left nephrostomy was placed. In a septic patient with obstruction, a percutaneous nephrostomy is safer than a double J stent.
![]() A 50-year-old homeless woman presents with gross hematuria and severe dysuria. This KUB was obtained as part of the initial workup. What is the significant radiographic finding?
A 50-year-old homeless woman presents with gross hematuria and severe dysuria. This KUB was obtained as part of the initial workup. What is the significant radiographic finding?

This KUB shows a retained ureteral stent with a large bladder calculus incorporated into the distal coil. Further questioning this patient revealed a history of ureterolithiasis and ureteral stent placement at an outside facility 18 months ago. It is imperative to secure follow-up in all patients with ureteral stents. The management should be based on functional findings on the right kidney with a study such as a diuretic renogram.
![]() A 30-year-old female involved in a motor vehicle accident presents with gross hematuria and underwent an IVU. What is the significant finding on the IVU?
A 30-year-old female involved in a motor vehicle accident presents with gross hematuria and underwent an IVU. What is the significant finding on the IVU?

The IVU shows a pelvic fracture with obvious displacement of the SI joint on the right. It is important on any film presented to look at surrounding structures. Be especially careful if you are given only one film from a series to review. In this case, the Foley catheter has already been successfully placed. A cystogram and drainage film did not show any evidence of bladder rupture.
![]() A 75-year-old female is evaluated for an episode of gross painless hematuria. The IVU obtained is significant for 2 abnormalities. Identify these problems.
A 75-year-old female is evaluated for an episode of gross painless hematuria. The IVU obtained is significant for 2 abnormalities. Identify these problems.

In elderly patients, it is especially important to look for associated findings. In this film, the left ureter deviates laterally in the upper third. There is a fine rim of calcification and a suggestion of a midline mass. On the left side, these findings are suspicious for an aortic aneurysm, which this proved to be. In addition, there is a large calcified pelvic mass displacing the bladder, which ultimately proved to be a Brenner tumor of the ovary. Not well seen is the invasive transitional cell carcinoma of the bladder, which was diagnosed by cystoscopy. Always remember that finding renal pathology does not exclude bladder and lower urinary tract pathology.
![]() A 40-year-old man undergoes an IVU to evaluate microhematuria. The 15-minute film is shown. What is the abnormality shown?
A 40-year-old man undergoes an IVU to evaluate microhematuria. The 15-minute film is shown. What is the abnormality shown?

Close inspection of the IVU shows a portion of a calyceal system just below the right pelvic brim and overlying the sacrum. This is an example of an ectopic kidney. The plain film in this case demonstrated a stone in the pelvic kidney. Up to 50% of pelvic kidneys will have hydronephrosis or reflux.
![]() A 42-year-old man who presented with a history of a febrile UTI was evaluated with an IVU. What is the likely diagnosis?
A 42-year-old man who presented with a history of a febrile UTI was evaluated with an IVU. What is the likely diagnosis?

This is an IVU that we do not often see in adults. There is duplication of the collecting system on the left. Duplication of one collecting system should immediately raise suspicion about duplication in the other kidney. The right collecting system is notable for only 2 major infundibula and tilts to the right, a finding labeled as the “drooping lily” sign. The collecting system is missing the upper pole calyx, which often bears close resemblance to a “ball peen hammer.” Additionally, there is a large lucent smooth filling defect in the bladder, which could be confused with a tumor or benign prostatic hypertrophy (BPH). However, putting the whole picture together, it is likely that this is an ectopic ureterocele with obstruction of an upper pole ureter in a complete duplication on the right. Ectopic refers to the location of the ureteral orifice, which is likely to be outside the trigone. The Meyer–Weigert rule governing the configuration of duplicate orifices is “the upper pole drains lower and lower pole drains lateral.” The lower pole orifice is located more laterally on the trigone and is therefore more prone to reflux, while the upper pole orifice enters more medially and is more often obstructed, ectopic, or associated with a ureterocele.
![]() A 27-year-old man presents with right flank pain. His urinalysis shows 0 RBCs/hpf, 2 to 4 WBCs/hpf, and no bacteria. An IVU is ordered. A delayed film of the IVU is shown. The left kidney was normal on the earlier films. Also a film from a later retrograde ureteropyelography is shown. What radiographic diagnosis is most likely?
A 27-year-old man presents with right flank pain. His urinalysis shows 0 RBCs/hpf, 2 to 4 WBCs/hpf, and no bacteria. An IVU is ordered. A delayed film of the IVU is shown. The left kidney was normal on the earlier films. Also a film from a later retrograde ureteropyelography is shown. What radiographic diagnosis is most likely?

The IVU shows massive hydronephrosis on the right side with no hydroureter, an appearance consistent with an ureteropelvic junction obstruction. A Lasix renogram may give a better estimate of relative function and degree of obstruction but, more importantly, may give a more sensitive test to use to assess outcome after repair. Retrograde ureteropyelography confirms the diagnosis. Many times the formal repair is done in the same setting as the cystoscopy with retrogrades.
![]() A retrograde pyelogram was attempted in a 10-year-old male with intermittent flank pain and hydronephrosis on ultrasound. The ureter is incompletely filled. What is the diagnosis?
A retrograde pyelogram was attempted in a 10-year-old male with intermittent flank pain and hydronephrosis on ultrasound. The ureter is incompletely filled. What is the diagnosis?
This film shows the classic appearance for a distal adynamic segment associated with a primary obstructed megaureter. The pathology is believed to be due to disordered smooth muscle in the distal segment of the ureter associated with increased collagen deposition. This segment fails to conduct the peristaltic wave and creates a functional obstruction. A similar mechanism is postulated for the majority of ureteropelvic junction (UPJ) obstructions.
![]() A 30-year-old man presented with right-sided flank pain. His urinalysis showed 0 RBC/hpf. An IVU was obtained. A 10-minute film is shown. What are the 2 likely diagnoses?
A 30-year-old man presented with right-sided flank pain. His urinalysis showed 0 RBC/hpf. An IVU was obtained. A 10-minute film is shown. What are the 2 likely diagnoses?

The lower pole of the left kidney has a medially based calyx, which is suggestive of a horseshoe kidney. In addition, the renal axis is shifted laterally. Approximately one-third of horseshoe kidneys may have a contralateral ureteropelvic junction obstruction. The renal pelves are oriented anteriorly, so the pyeloplasty is performed transabdominally. Ureterolithiasis with hydronephrosis is a possibility, but no stone is seen and the patient had no significant hematuria making this diagnosis less likely. A retrograde pyelogram at the time of surgery would confirm the diagnosis and rule out a stone or distal adynamic segment.
![]() An IVU was obtained to evaluate microhematuria in a young man. The radiographic diagnosis is?
An IVU was obtained to evaluate microhematuria in a young man. The radiographic diagnosis is?
While a medially based calyx is suggestive of a horseshoe kidney, here is the exception. The left kidney has medial calyces, but the right does not. This is a malrotated left kidney. The renal pelvis is oriented anteriorly during renal ascent and the kidney then rotates medially. Most malrotated kidneys rotate laterally instead so the vessels cross anteriorly.
![]() A retrograde pyelogram was obtained to evaluate an abnormality seen on IVU for microhematuria. A representative film is shown. What is the abnormality?
A retrograde pyelogram was obtained to evaluate an abnormality seen on IVU for microhematuria. A representative film is shown. What is the abnormality?
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


