Fig. 7.1
Pringle maneuver
“Simple hemi-occlusion” was created by Yan [12, 13] in 1994 and now is routinely used in our center.
The general steps are as described below:
We did not dissect hepatoduodenal ligament. Following the direction of the common hepatic duct, the confluence of the right and left portal pedicles would be found. After that an incision would be drawn on the liver capsule overlying the confluence using electrocautery (Fig. 7.2).

Fig. 7.2
On the visceral envelope overlying the confluence, a small hole was made using a sharp blade
Then we inserted a right-angle pliers in the incision to gently mobilize the liver substance outside Glisson’s sheath. The right-angle pliers should mobilize in the liver parenchyma toward the liver caudate lobe and there is no resistance (Fig. 7.3).

Fig. 7.3
A right-angle forceps was inserted to gently mobilize the liver parenchyma outside Glisson’s sheath
Finally the sharp end of the right-angle pliers would come out from the junction of portal vein and liver caudate lobe (Fig. 7.4).
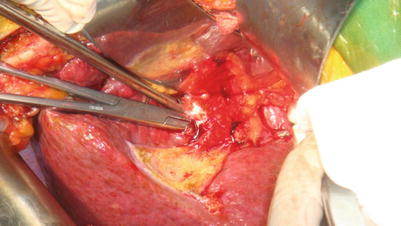
Fig. 7.4
The right-angle forceps should mobilize in the liver parenchyma toward the caudate lobe
In the meanwhile, a catheter was then wrapped around the right side branch of the portal pedicle through the incision (Fig. 7.5).
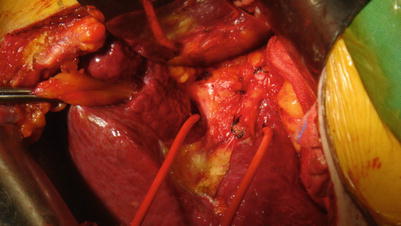
Fig. 7.5
A catheter was introduced
Tightening the catheter, the right hemihepatic vascular inflow would be occluded (Fig. 7.6) and the color in the hepatic surface is changed (Fig. 7.7).

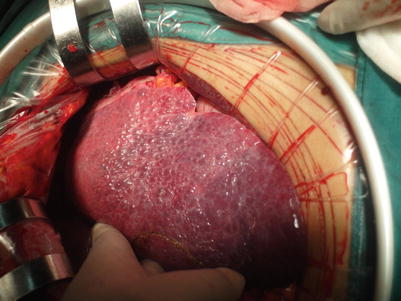
Fig. 7.6
Tightening the catheter
Fig. 7.7
The color in hepatic surface is changed
When put on one side of the catheter through the foramen of Winslow and then come out from the ligamentum hepatogastricum, tightening the catheter would result in occluding the left hemihepatic vascular inflow. In this method, intermittent vascular occlusion was not applied (Fig. 7.7).
“Hooking with ligation” is a simple and effective technique for liver resection created by Yan in 1994 [12, 13] and now is routing used in our center.
The surgical procedure is described below:
The resection line was marked by electrocautery on the hepatic surface before hepatectomy (Fig. 7.8).
Fig. 7.8
 Liver Anatomy and the History of Hepatectomy
Long-Term Outcomes of Liver Resection
Liver Anatomy and the History of Hepatectomy
Long-Term Outcomes of Liver Resection
 Pediatric Living Donor Liver Transplantation
Pediatric Living Donor Liver Transplantation
 Associating Liver Partition and Portal Vein Ligation for Staged Hepatectomy
Associating Liver Partition and Portal Vein Ligation for Staged Hepatectomy
 Procurement of Liver Graft
Procurement of Liver Graft
 Surgical Treatment of Hepatocellular Carcinoma Accompanied with Portal Vein Tumor Thrombus
Surgical Treatment of Hepatocellular Carcinoma Accompanied with Portal Vein Tumor Thrombus




The resection line was marked by electrocautery on the hepatic surface
Related posts:
Liver Anatomy and the History of Hepatectomy
Long-Term Outcomes of Liver Resection
Pediatric Living Donor Liver Transplantation
Associating Liver Partition and Portal Vein Ligation for Staged Hepatectomy
Procurement of Liver Graft
Surgical Treatment of Hepatocellular Carcinoma Accompanied with Portal Vein Tumor Thrombus
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
