Chapter 53 Surgery for Male Infertility
INTRODUCTION
Infertility affects at least 15% of all couples, and male factor is involved in approximately half of these cases. Approximately half the men with male factor infertility will have problems that are surgically correctable: 40% of men will have a varicocele and 15% will have an obstruction, including those with a previous vasectomy.1 Treatment of surgically correctable male factors is cost-effective and can spare the female partner invasive procedures and potential complications associated with the use of assisted reproductive technologies.2–4
Detection of surgically correctable problems requires an appropriate male factor evaluation, including a history, physical examination, and at least two semen analyses. Further testing, such as endocrine or genetic testing, may be required, depending on the results of the preliminary evaluation. In addition to diagnosing correctable problems, some men may have significant underlying medical problems diagnosed during their evaluation.5,6
DIAGNOSTIC PROCEDURES
Transrectal Ultrasound
Ejaculatory duct obstruction is a rare cause of infertility, accounting for less than 1% of cases. Causes include congenital atresia or stenosis; utricular, müllerian, or Wolffian duct cysts; trauma; and infection. A seminal vesicle diameter of greater than 1.5cm is suggestive of ejaculatory duct obstruction, although there is no definite threshold for making the diagnosis.7–10
A partial form of ejaculatory duct obstruction may to be present in men with low semen volume and severe oligoasthenospermia. According to some investigators, this condition can be detected by transrectal ultrasound. However, no precise criteria for diagnosing partial ejaculatory duct obstruction is available, and currently this condition is considered investigational.7
Testis Biopsy
The indications for a diagnostic testis biopsy are azoospermia with at least one palpable vas deferens.10–12 It must first be verified that the patient is indeed azoospermic by centrifuging the sample, resuspending the pellet, and repeating the microscopic examination.13 The primary purpose of a testis biopsy is to differentiate obstructive from nonobstructive azoospermia. Pathologic analysis should be performed to analyze the pattern of sperm production and to rule out intratubular germ cell neoplasia, which may occur in 0.4% to 1.1% of infertile men.10 Fixatives such as Bouin’s or zinc formalin allow for maintenance of the testicular architecture for pathologic examination.
A diagnostic classification system devised by Levin is useful in describing the pattern of sperm production.14 In the setting of azoospermia, more than 20 mature spermatids per tubule on histologic examination would be consistent with a sperm concentration of 10 million/mL, suggesting obstruction.15
The technique of diagnostic testis biopsy is straightforward. It can be performed through a small scrotal incision with local, regional, or general anesthesia on an outpatient basis. Delivery of the testis is usually not required for a standard biopsy. A biopsy can also be performed percutaneously with a biopsy gun or by fine-needle aspiration, although fewer tubules are obtained this way.16,17 To avoid injury to significant branches of the testicular artery, the biopsies should be taken from the medial or lateral aspect of the upper pole.18
If the testes are symmetric, a unilateral biopsy is sufficient to document obstruction. Bilateral biopsies are more important when attempting to maximize the chances for sperm retrieval.19
Vasography
The purpose of a vasogram is to assess the patency of the vas deferens. The indications for vasography are azoospermia, a normal FSH, a testis biopsy with normal spermatogenesis, and at least one palpable vas deferens.10,12
Virtually all vasal obstructions are iatrogenic. Vasal obstruction can be encountered after inguinal hernia repair or orchidopexy, retroperitoneal surgery such as renal transplantation and, of course, vasectomy. Vasography is not routinely necessary at the time of vasectomy reversal, however. Azoospermic men with normal semen volume, normal spermatogenesis on a testis biopsy, palpable vasa, and no history of inguinal, scrotal, or retroperitoneal surgery will most likely have epididymal obstruction.
Vasography can be performed with either a hemivasotomy or a puncture technique and should be performed only at the time of a planned reconstruction. The puncture technique is technically more difficult to perform. The advantage of the puncture technique is that it does not require separate closure of the vas deferens.20
If there is no difficulty with the injection, one can assume that the vas distal to the injection site is patent.10 A normal x-ray vasogram should demonstrate a barely perceptible but patent vasal lumen coursing from the scrotum through the inguinal canal to the pelvis, with filling of the ejaculatory ducts and bladder.
TREATMENT OF ACQUIRED OBSTRUCTION
Inguinal Vasal Obstruction
Obstruction of the vas deferens can occur after inguinal, scrotal, and retroperitoneal surgery.21 Reconstruction of the retroperitoneal vas is usually not possible secondary to retraction of the distal end, and reconstruction of the inguinal vas is challenging and in some cases not possible.
Inguinal vasal reconstruction begins with mobilization of the two ends of the vas deferens followed by a microsurgical anastomosis with either a modified one-layer or formal two-layer technique. Difficulties encountered with inguinal vasal reconstruction stem from the inability to isolate and mobilize the distal (abdominal) end and the dense scarring that occurs, particularly with mesh, after inguinal hernia repairs.22,23
In cases where there is inguinal vasal obstruction on one side and an atrophic testis with a normal ductal system on the contralateral side, strong consideration should be given to a trans-septal or “crossover” vasovasostomy because this is technically less complicated than performing an inguinal dissection and anastomosis. Sperm retrieval and in vitro fertilization with intracytoplasmic sperm injection (IVF/ICSI) should be considered as an alternative.24
Vasectomy Reversal
Vasectomy is one of the most popular forms of contraception and as many as 4% to 10% of men who undergo a vasectomy request a reversal.24 This procedure is performed as an outpatient with local, regional, or general anesthesia. Secondary epididymal obstruction can occur; in these cases vasoepididymostomy, rather than vasovasostomy, is required.25 Vasoepididymostomy is significantly technically more demanding than vasovasostomy. Vasovasostomy and vasoepididymostomy are usually performed through bilateral high scrotal incisions.
Vasovasostomy
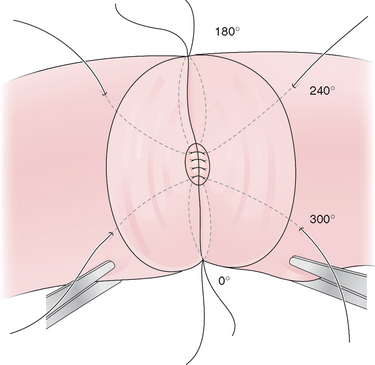
The vasal anastomoses can be performed with either a modified one-layer technique with 9-0 nylon or a formal two-layer technique with 10-0 and 9-0 nylon (Figs. 53-1 and 53-2).26 With the modified one-layer technique, four to six full-thickness 9-0 nylon sutures are placed with four to six 8-0 or 9-0 nylon sutures in the muscularis in between the full-thickness sutures. In the formal two-layer technique, the vasal mucosa is reapproximated as a separate layer with interrupted 10-0 nylon and the muscularis with 9-0 nylon.27
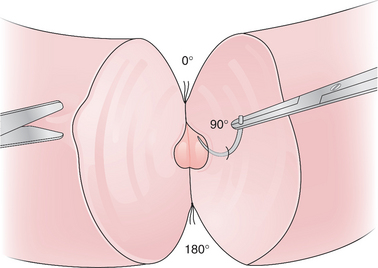
Figure 53-1 Vasovasostomy; modified one-layer technique. Four to six full-thickness nylon sutures are placed.
Vasoepididymostomy
The initial approach for vasoepididymostomy is similar to that for vasovasostomy. If thick, pasty vasal fluid without sperm is noted, vasoepididymostomy should be considered. The incisions are extended and the tunica vaginalis is opened to deliver the testis and spermatic cord. Typically, the site of epididymal obstruction can be identified by its distension and bluish brown discoloration. The vas deferens is mobilized distally to allow for sufficient length to reach the epididymis. This can require dissection up to the external ring with extension of the incision superiorly.
The vas deferens is then routed behind the cord to lie next to the epididymis and aligned with the epididymal tubule by placing 9-0 nylon sutures from the tunica of the epididymis to the muscularis of the vas deferens. In the traditional end-to-side technique five to eight 10-0 nylon sutures are placed into the open epididymal tubule and then to the mucosa of the vas deferens. The outer layer of the anastomosis is then completed by anastomosing the remainder of the epididymal tunic to the muscularis of the vas deferens with 9-0 nylon (Fig. 53-3).28 The scrotum is then closed in layers with absorbable suture.29
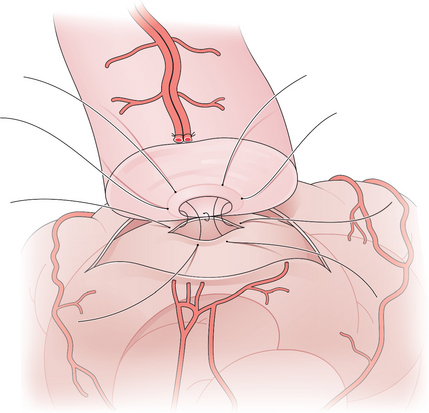
Figure 53-3 Vasoepididymostomy. A single epididymal tubule has been opened and sutured to the mucosa of the vas.
Newer techniques for vasoepididymostomy involve intusussception of the epididymal tubule into the lumen of the vas deferens. A triangulation technique with three double-arm 10-0 sutures was described by Berger and a two-suture technique was described by Marmar. With these techniques, the double-arm sutures are placed in the distended epididymal tubule before it is opened. The tubule is opened between the previously placed double-arm sutures and these are then placed in the corresponding position of the mucosa of the vas deferens. The outer layer of the anastomosis is completed with 9-0 nylon sutures from the tunica of the epididymis to the muscularis of the vas deferens.
The main advantages of these newer intusussception techniques are that the 10-0 sutures are easier to place in a distended tubule and the intusussception of the epididymis into the lumen of the vas deferens may reduce leakage. Patency may occur sooner than with traditional vasoepididymostomy, but pregnancy data for these newer techniques are generally lacking.30,31
Postoperative Course
The first semen analysis is checked between 4 and 12 weeks postoperatively and every 3 months thereafter. It can take as long as 6 months to see sperm return to the semen after vasovasostomy, and the average time to pregnancy is 1 year.32,33 It is not unusual to see lower sperm concentration and motility with the initial semen analyses, and it may take 3 to 6 months or longer to see the semen parameters reach a plateau.
Secondary restenosis of the anastomoses can occur in about 10% of cases with subsequent azoospermia.32,34 Sperm cryopreservation can circumvent this problem, but most men will not need the frozen sperm. After vasoepididymostomy, it can take as long as 1 year to see sperm return to the semen.32
Success Rates
Patency rates for vasovasostomy and vasoepididymostomy range from 75% to 93% and 67% to 85%, respectively. Patency rates depend on the obstructive interval (time since the vasectomy), the quality of the vasal fluid noted at surgery, whether epididymal obstruction is present, and surgical technique. Although vasovasostomy can be performed without an operating microscope, microsurgical technique generally yields superior results.35 Accurate performance of vasoepididymostomy without microsurgery would be essentially impossible.
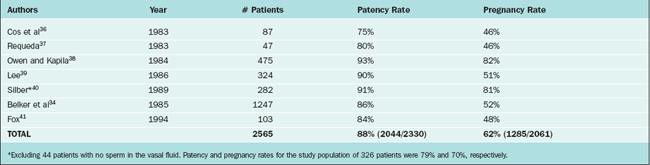
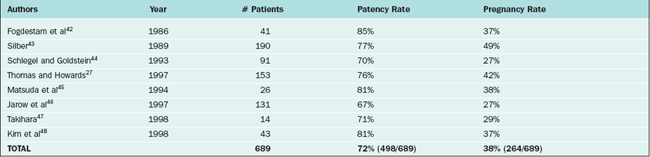
Pregnancy rates for vasovasostomy and vasoepididymostomy range from 46% to 82% and 27% to 49%, respectively27,33,36–48 (Tables 53-1 and 53-2). Pregnancy rates depend on the above variables as well as female factors and other factors such as antisperm antibodies.
In the study by the Vasovasostomy Study Group, a group of experienced microsurgeons examined the effect of obstructive interval and vasal fluid quality on patency and pregnancy rates. They clearly demonstrated that patency and pregnancy rates were inversely related to the obstructive interval. Patency and pregnancy rates were 97% and 76%, respectively, for obstructive intervals of 3 years or less, 88% and 53% for 3 to 8 years, 76% and 44% for 9 to 14 years, and 71% and 31% for 15 years or greater.
Vasal fluid quality, both the gross and microscopic appearance, was also an important prognostic factor. The patency and pregnancy rates for grossly clear fluid were 91% and 49%, repectively, for opalescent (cloudy, but thin and watery) fluid 93% and 59%, for thick/creamy fluid 70% and 45%, and for no fluid 88% and 54%. The patency and pregnancy rates were 94% and 63%, repectively, if motile sperm were present, 90% and 54% for nonmotile sperm, 96% and 50% for mostly sperm heads but some with tails, 75% and 40% for sperm heads only, and 60% and 31% if sperm were absent. Thus, the absence of sperm in the vasal fluid significantly lowers the success rate, but patency and pregnancy can still occur.33
If sperm are absent from the vasal fluid, epididymal obstruction may be present. Some investigators therefore recommend vasoepididymostomy if sperm are absent from the vas fluid, regardless of other factors. In a series of 44 patients with intravasal azoospermia, all patients remained azoospermic postoperatively. It was concluded that vasoepididymostomy should be performed if sperm are absent from the vas fluid.40 In the Vasovasostomy Study Group, the patency and pregnancy rates if sperm were absent in the vas fluid were 60% and 31%, respectively. Because epididymal obstruction is more likely to occur as the obstructive interval increases and thicker vasal fluid is more suggestive of epididymal obstruction, it is possible to apply vasoepididymostomy selectively and still obtain acceptable results. The Vasovasostomy Study Group recommended that vasoepididymostomy be considered if there was thick pasty fluid without sperm and the obstructive interval was 9 years or more.33 In another study, Kolettis and colleagues found that if vasovasostomy were applied in instances of intravasal azoospermia where the obstructive interval was 11 years or less, the patency and pregnancy rates were 80% and 38%, respectively, similar to those for vasoepididymostomy.49
TREATMENT OF OTHER FORMS OF OBSTRUCTION
Epididymal Obstruction
Epididymal obstruction can occur secondary to inspissated secretions in men with Young’s syndrome. This syndrome is characterized by a combination of obstructive azoospermia and chronic sinopulmonary infections in men without cystic fibrosis.10
If epididymal obstruction is suspected based on these clinical clues, the patient should be scheduled for testis biopsy, vasography, and possible bilateral vasoepididymostomy, all of which can be done at the same time. In these cases, the testis biopsy will document normal spermatogenesis. An intraoperative wet preparation of the biopsy will demonstrate the presence of significant numbers of sperm.50 Permanent pathology is required to document the pattern of sperm production. After vasography, a vasoepididymostomy can be performed. If the patient desires, simultaneous sperm retrieval can be carried out at the same time.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


