Chapter 44 Gynecologic Laparoscopy
HISTORY
The first experimental laparoscopy (ceolioscopy) was performed by Dr. Georg Kelling in Berlin in 1901; Kelling placed a cystoscope into the abdomen of dogs to evaluate the ability of insufflated air to stop gastrointestinal hemorrhage.1 Dr. Hans Christian Jacobaeus of Sweden published the first description of laparothoroscopy in 1910 as a technique to evaluate patients with peritoneal tuberculosis. However, laparoscopy made little headway into clinical practice until after World War I. It took until the 1960s for laparoscopy to be accepted in the United States and Europe as a safe and valuable surgical procedure.
For many years, gynecologic laparoscopy was performed almost exclusively for diagnostic purposes and for sterilizations. By the 1970s, the role of laparoscopy had expanded to include lysis of adhesions and treatment of endometriosis.2 The technology and equipment advanced over the next three decades such that laparoscopy is now used for a wide variety of procedures ranging from treatment of ectopic pregnancies and ovarian cysts to hysterectomy, incontinence procedures, and management of gynecologic malignancies.
GENERAL TECHNIQUES FOR LAPAROSCOPY
Primary Trocar Placement
Standard Closed Technique: Veress Needle and Primary Trocar Insertion
The standard closed technique was used almost exclusively for decades and continues to be widely used today. Both the Veress needle and primary trocar are blindly placed through a periumbilicar incision into the peritoneal cavity. Using this approach with reusable instruments, the combined risk of injuring retroperitoneal vessels, bladder, or bowel has been found to be less than 1 in 1000 cases.3 This approach has become the gold standard against which all other techniques are judged.
In a woman of ideal weight (body mass index [BMI] <25kg/m2) or only slightly overweight (BMI 25 to 30kg/m2), the lower anterior abdominal wall is grasped and elevated, and the Veress needle is inserted toward the hollow of the sacrum at a 45-degree angle (Fig. 44-1).4 In the thinnest patients in this group, the retroperitoneal vessels are much closer to the abdominal wall and the margin for error is reduced, with as little as 4 cm between the skin and these vessels. In the obese patient (BMI >30kg/m2; weight usually greater than 200 pounds), a more vertical approach, approximately 70 to 80 degrees, is required to enter the peritoneal cavity because of the increased thickness of the abdominal wall.
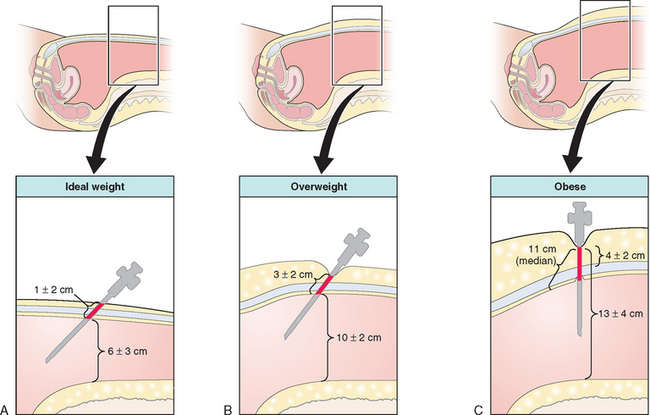
Verification that the Veress needle tip is in the peritoneal cavity is done by a number of methods, including the hanging drop test, injection and aspiration of fluid through the Veress needle, and close observation of intra-abdominal pressure during carbon dioxide insufflation. After a pneumoperitoneum has been created, the Veress needle is removed and the primary port trocar (most commonly 5 or 10 mm in diameter) is placed at an angle identical to that used for the Veress needle.
Direct Trocar Insertion
Direct trocar insertion is a technique whereby the primary trocar is inserted without the Veress needle being previously inserted and insufflating the abdomen with carbon dioxide.5 The primary trocar is inserted at an angle similar to that described for the closed technique. The peritoneal cavity is then insufflated with carbon dioxide through the umbilical port. This technique decreases the risk of extraperitoneal insufflation by allowing the surgeon to confirm intraperitoneal placement of the primary trocar before insufflation. Although small randomized studies have not demonstrated an increased risk of injuries, some series suggest that this technique might increase the risk of bowel injury.5,6 Further large studies are required.
Open Laparoscopy
Open laparoscopy, first described by Dr. Harrith Hasson in 1971, refers to creating a small incision in the abdomen and placing the port through the incision without using a sharp trocar.7,8 The skin and anterior rectus fascia are incised with a scalpel and the peritoneal cavity is bluntly entered with a Kelly or Crile forceps. A laparoscopic port with a blunt-tipped trocar is then placed into the peritoneal cavity. For the Hasson technique, fascial sutures are used to help maintain a pneumoperitoneum.7 This method almost completely avoids the risk of retroperitoneal vessel injury and is preferred by many laparoscopists for this reason. Although open laparoscopy does not entirely avoid the risk of bowel injury, many laparoscopists use this approach in an effort to decrease this risk in patients with previous abdominal surgery suspected of having adhesions.
Left Upper Quadrant Technique
It is important to know the anatomy of the left upper quadrant before using this technique. The most important organs that are closest to this site are the stomach and left lobe of the liver.9 Although a small series has shown the risk of complications to be small, the relative risk of complications with this technique remains to be demonstrated by a large study.10
Placement of Secondary Ports
Secondary ports are required to perform most gynecologic laparoscopy procedures today. After identifying the inferior epigastric vessels by visualizing them intra-abdominally through the laparoscope, one to three secondary ports are placed, depending on the procedure.11 A midline port may be placed 3 to 4 cm above the pubic symphysis. Lateral ports are placed approximately 8 cm from the midline and above the pubic symphysis to avoid the inferior epigastric vessels (Fig. 44-2).12 This lateral site corresponds to McBurney’s point in the right lower quadrant, and is approximately one-third the distance from the anterior iliac crest to the pubic symphysis (see Fig. 44-2). An additional lateral port for the principal surgeon is required for most operative laparoscopy cases. The site chosen is typically at the level of the umbilicus lateral to the rectus muscle. This site offers the surgeon comfortable use of both hands and allows access to most areas of the pelvic or abdominal cavity.
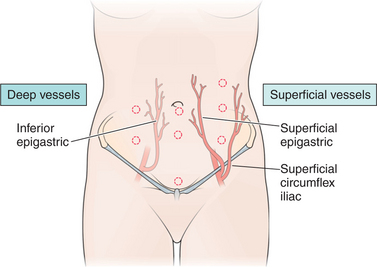
Figure 44-2 Ideal port sites in relation to the deep and superficial vessels of the anterior abdominal wall.
Removal of Ports and Port Site Closure
It has become clear that large port sites are at a small but undeniable risk for subsequent bowel herniation if not securely closed.13 Furthermore, patients with ascites or in whom intra-abdominal fluid has been placed for chemotherapy or adhesion prevention are at risk of postoperative leakage through the port site. For these reasons, it is recommended that all extra-umbilical port sites be surgically closed when a trocar greater than 8 mm in diameter was used for port placement or if repeated removal and replacement of the port has enlarged the fascial defect. Although the risk of herniation at the umbilicus appears to be extremely rare, some surgeons recommend closing the fascia at this site as well.
Closure of lateral ports is more of a challenge because the fascia is clearly divided into sheaths. Closure of only one fascial sheath puts the patient at risk of herniation of bowel between the sheaths, often referred to as a Spigelian hernia (see Chapter 45). For this reason, methods have been designed to simultaneously close both layers.
When closing secondary ports, it is imperative to do so under direct laparoscopic visualization to avoid bowel injury. One of several transabdominal suture guides are used to place interrupted absorbable suture through both the anterior and posterior fascial sheaths, usually incorporating the peritoneum as well. However, even this technique does not completely prevent subsequent herniation.14 For this reason, any painful bulge appearing beneath a laparoscopic port site should be evaluated ultrasonographically to detect bowel herniation.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


