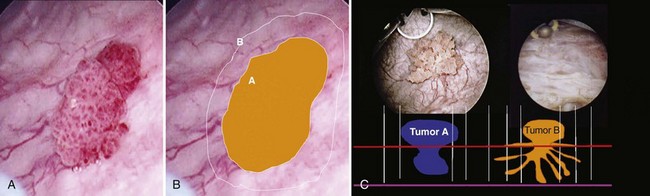
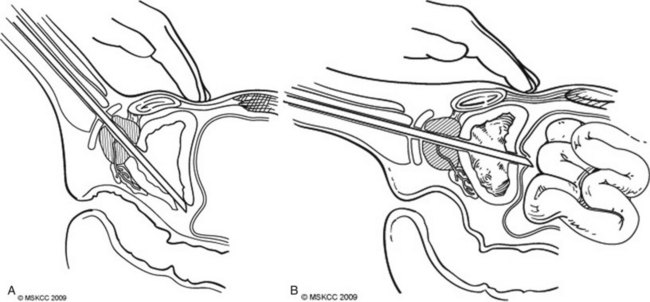
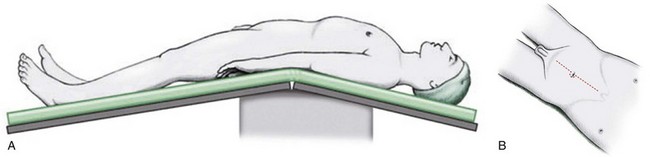
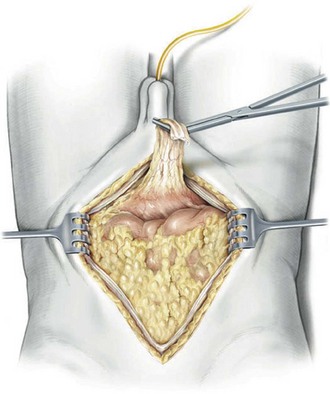
Ryan Kent Berglund, MD, Harry W. Herr, MD According to the American Cancer Society, cancers of the urinary bladder accounted for an estimated 70,980 new cases and 14,330 deaths in the United States in 2009 (Jemal et al, 2009). These cancers are the sixth leading cause of cancer death among Americans, and they are a significant source of health care costs. The first publication of long-term outcomes using the techniques of radical surgery with wide local excision and removal of regional lymph nodes with urinary diversion came from Whitmore and Marshall (1962). In their landmark publication, they observed 5-year survival rates of 21% to 49% in their series of 230 patients. Since then, advances in endoscopic and open surgical technique, as well as perioperative care, have reduced the surgical mortality from more than 10% to less than 5% and improved results. Additionally, the use of neoadjuvant chemotherapy treatment before surgery has led to increased long-term survival. Recent large series have shown 10-year cancer-specific survival rates in patients with pathologic T2 cancers of 65% to 78% (Stein et al, 2001; Shariat et al, 2006). Once the tumor or tumors are identified, resection is performed using a cutting current on the loop resection device down to the level of the detrusor muscle. It is essential to resect to this depth to obtain sufficient tissue for pathologic staging and for completeness of resection (Fig. 83–1). The margin of resection should include a 2- to 3-cm visually negative margin as deep muscle spread of tumor can occur in either a broad-based or tentacular fashion (Fig. 83–2). Resection of tumors involving the lateral bladder wall risk stimulation of the obturator nerves, leading to rapid thigh adduction and possible perforation of the bladder. This can be minimized by reducing the cautery current and rapidly tapping the foot pedal. Smaller and multiple lesions can be treated with cold cup biopsy and fulguration or fulguration alone on a coagulation current, or with another energy source such as a neodynium-yttrium-aluminum garnet laser (Nd : YAG). Bladder perforation is a complication that occurs in resections carried to the optimal depth of resection into the detrusor muscle. On the basis of the location of the perforation, these result in either an extravesical or intravesical extravasation of irrigant. Perforations that occur at the trigone, bladder base, and laterally typically result in an extravesical perforation with irrigant extravasation and can often be managed conservatively with Foley catheter drainage (Fig. 83–3A). Perforations at the bladder dome can result in intraperitoneal perforation and extravasation and often require operative repair and drainage of irrigant (Fig. 83–3B). Intraperitoneal ruptures are often diagnosed intraoperatively with palpation of the abdomen confirming distension from irrigant. An intraoperative cystogram can confirm rupture of either type. Following resection without bladder perforation, instillation of intravesical chemotherapy with agents such as doxorubicin or mitomycin-c can modestly reduce recurrence rates from 15% to 38% but have little effect on progression (Kurth et al, 1997; Huncharek et al, 2001). Instillation of BCG, which is reserved for superficial high-grade disease, has shown superior efficacy in both recurrence rates and progression but should be instilled 2 to 4 weeks after resection due to the potential risks of “BCG-osis” with a disrupted urothelium (Lamm et al, 1991). The patient is positioned in the supine position with the table flexed at the level of the anterior superior iliac spine of 15 degrees (Fig. 83–4). Spreader bars or low-lying stirrups are helpful, especially to facilitate access to the perineum in males or vaginal vault in females. The abdomen is prepared with a 10% povidone-iodine solution from below the xiphoid process to the upper thighs, with the perineum and inner thigh prepped as well. A vaginal prep should be done in the female patient. An incision is made in the midline from 2 cm above the umbilicus to the pubis, although in many cases the operation can be performed only through an infraumbilical incision, facilitating a faster recovery. The underlying anterior and posterior layers of the fascia are divided, and the extraperitoneal space is entered. The bladder is then mobilized to the pelvic side walls on both sides. Once this space is developed, a peritoneotomy is made and the peritoneum is entered. The urachal remnant is then encircled and divided near the level of the umbilicus (Fig. 83–5). The peritoneum is incised lateral to the medial umbilical ligaments to the internal inguinal rings bilaterally. The peritoneum overlying the bladder should always be removed with the specimen. The vas deferens is encountered and divided. At this time, the root of the small bowel mesentery is mobilized from the right lower quadrant to ensure appropriate exposure of the right ureter, gonadal vessels, and great vessels in preparation of the lymph node dissection, while the descending colon is mobilized laterally at the white line of Toldt (Fig. 83–6). A large peritoneal window is developed with the sigmoid colon to allow a sufficient gap through which the left ureter can pass for the urinary diversion.
Transurethral Resection of Bladder Tumors
Surgical Technique
Related posts:
 Definitive Therapy for Localized Prostate Cancer: An Overview
Definitive Therapy for Localized Prostate Cancer: An Overview
 Tuberculosis and Other Opportunistic Infections of the Genitourinary System
Tuberculosis and Other Opportunistic Infections of the Genitourinary System
 Surgical Procedures for Sphincteric Incontinence in the Male: The Artificial Genitourinary Sphincter and Perineal Sling Procedures
Surgical Procedures for Sphincteric Incontinence in the Male: The Artificial Genitourinary Sphincter and Perineal Sling Procedures
 Prosthetic Surgery for Erectile Dysfunction
Prosthetic Surgery for Erectile Dysfunction
 Neuropathic Dysfunction of the Lower Urinary Tract
Neuropathic Dysfunction of the Lower Urinary Tract
 Ectopic Ureter, Ureterocele, and Ureteral Anomalies
Ectopic Ureter, Ureterocele, and Ureteral Anomalies
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Abdominal Key
Fastest Abdominal Insight Engine