Right Anterior and Posterior Sectionectomy (Bisegmentectomy)
M.B. Majella Doyle
Adeel S. Khan
William C. Chapman
Introduction
The liver is comprised of eight anatomic segments that are defined by the distribution of the hepatic and portal venous system (Fig. 23.1). These segments can be grouped into four sections or sectors: The right anterior section (segments V and VIII), right posterior section (segments VI and VII), left medial section (segment IV), and left lateral section (segments II and III). Each segment is a functionally independent unit with its own vascular inflow, outflow, and biliary drainage. Consequently, it is possible to remove individual segments (and sectors) without disrupting the blood flow or biliary drainage of the remaining liver (see Chapter 24). Anatomic segment or sector based resections are not only just oncologically superior to non-anatomic resections but also allow for maximal conservation of normal liver parenchyma. In this chapter we will discuss our technique of right anterior and posterior sectorectomy.
 INDICATIONS/CONTRAINDICATIONS
INDICATIONS/CONTRAINDICATIONSIndications
The most common indication is resection of benign or malignant hepatic lesions that meet the criteria for resection (see Chapter 18) and involve all or part of segments V and VIII (anterior sector) or VI and VII (posterior sector). Less common indications include benign biliary strictures of the anterior or posterior sectoral bile duct or retroperitoneal tumors that involve the posterior sector secondarily.
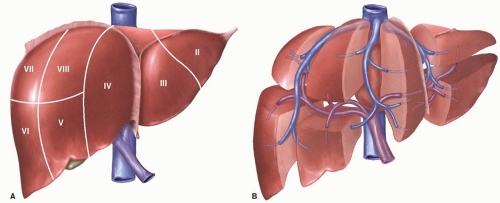 Figure 23.1 Diagrammatic representation of the segmental anatomy of the liver as defined by Couinaud. Segment I (Caudate lobe) is not seen. Each segment of the liver has its own vascular inflow (portal vein and hepatic artery), outflow (hepatic veins) and biliary drainage. This allows successful removal of individual segments (and sectors) without disrupting the blood supply to the remaining liver. LHV, left hepatic vein; MHV, middle hepatic vein; PV, portal vein; RHV, right hepatic vein. |
Contraindications
Absolute contraindications include presence of wide spread metastatic disease, advanced cirrhosis (Childs Pugh class C) or inability of the patient to tolerate general anesthesia.
 PREOPERATIVE PLANNING
PREOPERATIVE PLANNINGPreoperative investigation includes liver and renal function tests, complete blood count, and coagulation profile. All patients should have cross-sectional imaging either with a contrast-enhanced abdominal computed tomography (CT) scan or magnetic resonance imaging (MRI). The lesion under question must be localized to either right anterior or posterior sector and must be resectable (Figs. 23.2, 23.3). Invasion or thrombus of the portal vein outside the area of resection must be ruled out. An attempt should be made to assess the function of the remaining liver and evaluate for extent of cirrhosis, steatosis, or chemotherapy induced hepatic damage. Volumetric analyses may be necessary in these patients especially when additional hepatic resections are required. Older
patients and all patients with significant medical comorbidities must undergo thorough cardiopulmonary assessment and clearance before proceeding with surgery. At Washington University in St. Louis, an image-guided planning system to reconstruct the cross-sectional images as 3D images where the hepatic and portal veins are displayed along with the tumor and a resection plane can be drawn and manipulated to achieve the desired resection margin (Fig. 23.4). The future liver remnant (FLR) volume is also calculated in an automated fashion (see Chapter 18).
patients and all patients with significant medical comorbidities must undergo thorough cardiopulmonary assessment and clearance before proceeding with surgery. At Washington University in St. Louis, an image-guided planning system to reconstruct the cross-sectional images as 3D images where the hepatic and portal veins are displayed along with the tumor and a resection plane can be drawn and manipulated to achieve the desired resection margin (Fig. 23.4). The future liver remnant (FLR) volume is also calculated in an automated fashion (see Chapter 18).
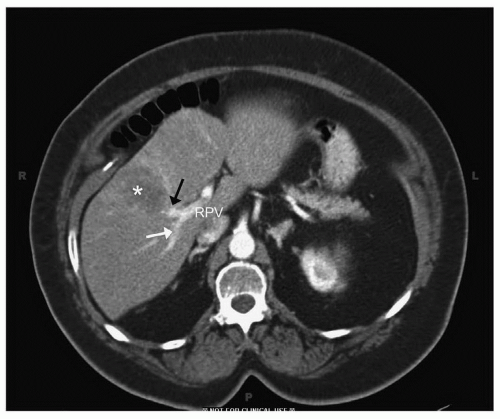 Figure 23.2 Computed tomography (CT) image of a patient with metastatic colon cancer to the right anterior sector. The classic hypo-attentuating lesion (asterix) can be seen in segment V. Note the relationship of the tumor with anterior (black arrow) and posterior (white arrow) sectoral branches of the right portal vein (RPV). |
 Figure 23.3 A: Computed tomography (CT) image of the patient with colorectal metastasis to the posterior sector of the liver. Small hypo-attenuating lesion (white arrow) can be seen in segment VII. Note the relationship with right hepatic vein (RHV). B: CT image of patient with sarcoma involving segment VII (asterix) seen posterior to the RHV. Note abutment of the tumor against the inferior vena cava (IVC). |
 SURGICAL TECHNIQUE
SURGICAL TECHNIQUEAnatomy
The liver can be divided into right and left hemi-livers by the middle hepatic vein, which runs in the mid-hepatic plane designated as “Cantile’s Line,” which runs from the gallbladder fossa to the suprahepatic vena cava. The right liver is further divided
into an anterior sector and a posterior sector by the right portal scissura containing the right hepatic vein (RHV). The anterior sector is made up of two segments—segment V caudally and segment VIII cranially. Similarly, the posterior sector comprised of segment VI caudally and segment VII cranially (see Fig. 18.6). All of these landmarks can be identified on intraoperative ultrasound, which should be an essential component of any major liver resection procedure. It is imperative that all hepatobiliary surgeons be very comfortable with this imaging modality (see Fig. 18.9).
into an anterior sector and a posterior sector by the right portal scissura containing the right hepatic vein (RHV). The anterior sector is made up of two segments—segment V caudally and segment VIII cranially. Similarly, the posterior sector comprised of segment VI caudally and segment VII cranially (see Fig. 18.6). All of these landmarks can be identified on intraoperative ultrasound, which should be an essential component of any major liver resection procedure. It is imperative that all hepatobiliary surgeons be very comfortable with this imaging modality (see Fig. 18.9).
 Figure 23.4 3D reconstruction image showing resection plane (white arrow) with heat map to calculate planned resection margin. Tumor location is marked with asterix. |
Positioning
The patient is positioned supine with arms in or out. All bony prominences are suitably padded.
Technique
Right Anterior Sectionectomy (Bisegmentectomy—Segments V and VIII)
1. Skin incision: The choice of incision depends on surgeon’s experience and comfort. Some of the commonly used incisions include unilateral or bilateral subcostal incision with midline extension, midline incision, or by a thoracotomy extension from right subcostal incision. We favor the right subcostal with midline extension (see Fig. 18.7) (see also Figs. 19.3 and 21.5) or bilateral subcostal with midline extension (“Mercedes Benz” incision).
2. Careful inspection of abdominal cavity to rule out extra hepatic disease.
3. Take down falciform ligament over anterior surface of the liver.
4. Perform intraoperative ultrasound (IOUS) of the liver to delineate vascular anatomy and relationship of the tumor with the hepatic veins and portal pedicles (Fig. 23.5). The RHV is identified at its point of entry into the vena cava and moving the probe caudally along the liver allows it to be followed into the hepatic parenchyma. The RHV separates the anterior sector from the posterior sector and therefore is an important landmark. It is important to check for a common variant where the anterior sector is drained by a large branch draining directly into the middle hepatic vein.
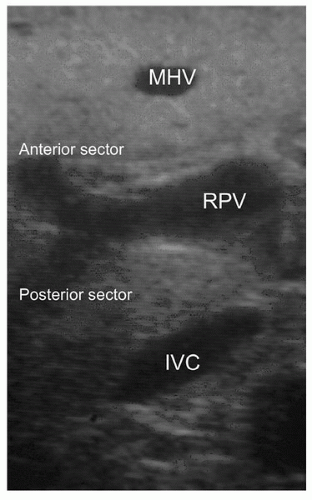 Figure 23.5 IOUS of the liver demonstrating relevant anatomy for right anterior and posterior sectoral resection. RPV can be seen bifurcating into anterior sectoral and posterior sectoral branches. MHV, Middle hepatic vein; IVC, inferior vena cava; RPV, right portal vein. |
 Figure 23.6 Circumferential dissection of RHV (white arrow). Lateral view; IVC, inferior vena cava; RHV, right hepatic vein. |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


