Clinical Staging
Cancers of the gallbladder are ultimately pathologically staged according to their depth of penetration and extent of spread. Clinical staging for GBC consists of imaging modalities as well as pathologic specimens when available from prior surgical resections.
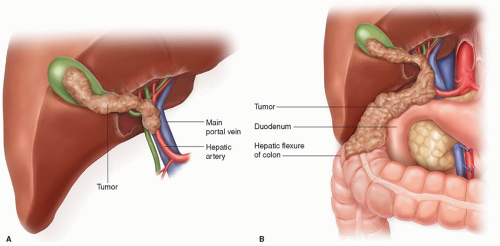
For GBC discovered by the pathologist incidentally, subsequent staging depends on pathologic tumor (T) stage. Extent of locoregional disease is directly correlated with the T stage of GBC, with more invasive lesions exhibiting higher rates of lymph node and distant metastases. T stage classification depends on the depth of tumor penetration into the wall of the gallbladder, on the presence of tumor invasion into the liver, hepatic artery, or portal vein, and on adjacent organ involvement. T1a lesions, those that have not breached the muscular layers, require no further staging or treatment. Accurate staging for more advanced, resectable tumors requires that all hilar lymph nodes be removed and analyzed. The hilar nodes include the lymph nodes along the common bile duct (CBD), hepatic artery, portal vein, and cystic duct.
For any tumor that has invaded the muscular layer or beyond, additional postoperative imaging is mandatory for clinical staging. This should include high-resolution 3D imaging of the chest, abdomen, and pelvis, specifically evaluating regional lymphadenopathy or any evidence of distant metastases. In addition, because even sophisticated imaging may understage disease and underestimate the propensity to seed the peritoneal surfaces after the prior operation, staging laparoscopy should be strongly considered. A minority of patients may present not with a tissue diagnosis, but with either (a) an incidentally found mass discovered while imaging the patient for other reasons, or (b) jaundice. Under these circumstances, in addition to the imaging studies described above, one should obtain a complete blood count (CBC), liver function tests, consider adding CA19-9 and carcinoembryonic antigen (CEA) serum markers, and again strongly consider staging laparoscopy, depending on results of the aforementioned tests.
 INDICATIONS/CONTRAINDICATIONS
INDICATIONS/CONTRAINDICATIONS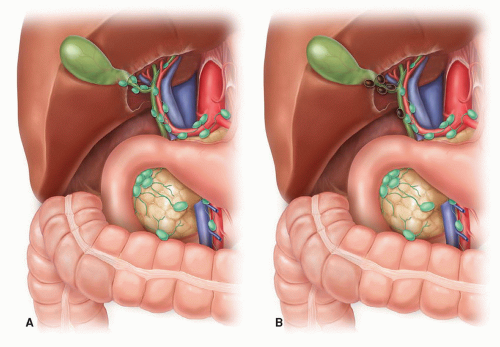
 PREOPERATIVE PLANNING
PREOPERATIVE PLANNING








