Chapter 66 Pyogenic liver abscess
Overview
Pyogenic liver abscess (PLA) may be defined as solitary or multiple collections of pus within the liver, the result of bacterial infection. In 1938, Ochsner and coworkers reported the first series of patients with hepatic abscesses in the modern surgical era treated by surgical drainage. This study included 47 patients and reported an overall survival of 67%. The advent of antibiotic therapy marked the basis of the contemporary treatment of liver abscesses, becoming a major part of the therapy, combined with surgical drainage. The first landmark report in minimally invasive treatment of liver abscess was that of McFadzean and colleagues in 1953. They presented a group of 14 patients who underwent percutaneous drainage for PLAs with no deaths within the group. Although potentially effective for dealing with the liver problem, such approaches present the disadvantage of overlooking the underlying abdominal pathology because of the lack of surgical exploration.
The development of clinical ultrasound (US) in the 1960s and the introduction of computed tomography (CT) in the 1970s represent the two major advances in the diagnosis and treatment of PLAs. Surgical exploration as a diagnostic tool was replaced by abdominal imaging, thus allowing minimally invasive techniques to become the first choice of treatment. Currently, percutaneous needle aspiration (PNA) and percutaneous catheter drainage (PCD) have become standard methods for both single and multiple PLAs (see Chapter 28). Surgical debridement, done either in an open or laparoscopic fashion, has a limited therapeutic role for patients in whom nonoperative treatment fails or in those requiring surgical treatment for the underlying cause of the abscess. In addition, surgical exploration may be indicated as the initial procedure when coexistence of peritonitis is suspected as result of abscess rupture into the peritoneal cavity.
Etiology
During the nineteenth century, PLAs were well known as a complication of acute appendicitis. Since then, etiology and presentation have dramatically changed. Inflammatory abdominal diseases are no longer the most common underlying conditions for PLAs, being replaced in later decades by a higher incidence of biliary causes, including malignancies, immunocompromised status, and advanced age (Branum et al, 1990). In 1996, Huang and colleagues (1996) presented a review that spanned more than 40 years in the treatment of PLAs. They analyzed and compared patterns of clinical presentation in 80 patients treated between 1952 and 1972 with a second group of 153 patients treated from 1973 to 1993. The authors concluded that the increased incidence of biliary malignancies as a cause of PLAs was due to a more aggressive approach in the treatment of this pathology, which includes more frequent instrumentation of the biliary tree (see Chapters 28 and 50D). Hilar cholangiocarcinoma was the most frequent single condition found during the second period reviewed, with the use of biliary stents and broad-spectrum antibiotics leading to the emergence of mixed bacterial and fungal infections. Biliary malignancy was an important risk factor for hospital mortality (Lok et al, 2008).
Elucidating the subjacent condition that caused a liver abscess is as important therapeutically as the correct treatment of a PLA. In a simplified schema, infection may get to the liver by five different avenues: 1) portal vein, 2) hepatic artery, 3) biliary tree, 4) adjacent organ infection, and 5) direct trauma to the liver. The term cryptogenic PLA applies when no underlying pathology is identified (Box 66.1).
Box 66.1 Classification of PLA According to the Underlying Mechanism of Dissemination
Portal pyemia is often a consequence of intraabdominal infection, such as acute appendicitis or diverticulitis. The incidence of this mechanism as a cause of PLA has markedly decreased in the past years. However, portal vein patency must be evaluated with Doppler US or dynamic CT scan in patients with PLAs. Gastrointestinal malignancies, such as colorectal adenocarcinoma or even gastric carcinoma, may also lead to a disruption of the mucosal barrier, leading to pyemia and liver abscess in the absence of liver metastasis (Tzur et al, 2003). This phenomenon should be particularly considered in the evaluation of patients with a cryptogenic PLA (Lim & Lim, 2004). Adequate investigation of etiology after PLA treatment may lead to a diagnosis of an underlying disease previously unknown for the patient (Mohsen et al, 2002).
Hematogenous spread of infection through the hepatic artery may also cause PLA. Frequent examples are bacterial endocarditis and intravenous drug abuse, but certain immunosuppressive conditions may also be associated with this mechanism. Liver cirrhosis is often associated with immunodeficiency, and the incidence of liver abscesses in cirrhotic patients compared with the general population is increased (see Chapter 9; Molle et al, 2001). Loss of hepatic filter function, impaired immunity, and frequent abdominal infections may also be responsible factors. Immunosuppressive drug use, alcoholism, chronic pancreatitis, pyelonephritis, and acquired immune deficiency syndrome are also associated with PLA (Huang et al, 1996).
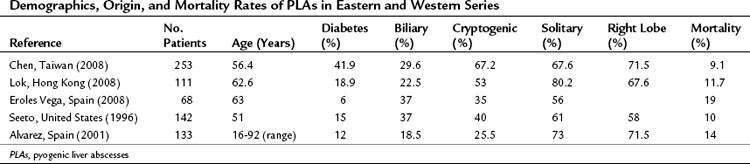
The incidence of diabetes mellitus varies among different series, but its presence is associated with a 10-fold increased risk for PLA compared with that of the general population. Diabetes mellitus was the most common comorbidity in a report of PLA from Taiwan and was present in 41 (16%) of 253 patients with PLA (Chen et al, 2008a). Biliary pathology has become the most identifiable cause of PLA in recent decades (Alvarez et al, 2001a). In this group of patients, infection may have different etiologies. Bile duct strictures, common bile duct stones, and hepatolithiasis are benign conditions that may cause PLA (see Chapters 43 and 44). Benign diseases are more commonly reported in Asia (Lok et al, 2008); in Western countries, however, biliary malignancy is a more prevalent condition. Instrumentation of bile duct obstruction by endoscopic stenting or percutaneous drainage is a frequent cause of cholangitis and PLA. Malignancy is a predictor of higher recurrence and mortality rates. The mortality rate of PLA caused by underlying malignant disease is almost twice as high as that of nonmalignant disease (Yeh et al, 1998).
Direct liver contamination by adjacent organ infection may produce a PLA, with acute cholecystitis being the most common example (see Chapter 31). However, gastric and duodenal perforation directly into the liver may also give rise to a PLA. Perforation secondary to foreign bodies, mainly from fish bones, have been also reported. In addition, liver parenchyma may become infected after direct damage. Intrahepatic biloma, hematoma, and necrotic parenchyma are favorable conditions for development of a PLA. This is a well-known consequence of blunt or penetrating liver trauma and liver resections.
In recent decades, local treatments for liver tumors have become a widespread alternative for many patients. These local techniques include ethanol injection, transarterial chemoembolization (TACE), selective internal radiation therapy, and radiofrequency ablation (RFA) (see Chapter 83, Chapter 84A, Chapter 84B, Chapter 85A, Chapter 85B, Chapter 85C, Chapter 85D ), which induce tumor necrosis either by chemical or thermal tissue destruction. In all these patients, PLA is a potentially life-threatening complication that may occur up to 5 months after a successful procedure. Transarterial liver embolization may be helpful in patients with hepatocellular carcinoma or liver metastases of gastrointestinal sarcomas and neuroendocrine tumors. The incidence of liver abscess after this procedure is low. Ong and colleagues (2004) reported PLAs in 0.26% of 3878 embolizations; the mortality rate in these patients was 33%. Patients with bilioenteric anastomosis are at particular risk for this complication. The odds ratio (OR) for developing PLA in this population was 894 in a series from Philadelphia (Kim et al, 2001). Subjacent pathology is not a predisposing factor for this complication (Song et al, 2001), but RFA of liver tumors may also cause a PLA. In a multicenter study from Italy, Livraghi and coworkers (2003) reported 2320 patients with 3554 lesions, with a 0.3% incidence of PLA. This incidence was slightly higher (1.7%) in another group of patients with hepatocellular carcinoma treated by RFA (Choi et al, 2005). De Baere and colleagues (2003) reported a 100% incidence of liver abscess in patients with prior bilioenteric anastomosis who underwent RFA. A further prospective analysis showed an incidence of PLA of 50% in patients with biliary diversions, but the risk was not increased if this diversion was performed synchronously with the ablation procedure (Elias et al, 2006).
In some patients with a PLA, no underlying cause is identified; they are considered to have a cryptogenic PLA. These cases account for up to 67% in some published data (Chen et al, 2008a). Etiology and presentation are summarized in Table 66.1.
Incidence
PLA is a rare disease, and actual incidence rates are poorly described in the literature. However, recent investigations demonstrated a marked increase of PLA incidence in the general population in the last few years. Huang and colleagues (1996) showed that PLA accounted for 13 per 100,000 hospital admissions in 1973, which increased to up to 20 per 100,000 only 20 years later. In a recent study from a teaching hospital in the United Kingdom, PLA had an incidence of 18.5 per 100,000 hospital admissions, with an estimated crude incidence of 2.3 cases per 100,000 the general population (Mohsen et al, 2002).
The second, a national series from Denmark (Jepsen et al, 2005), analyzed 1448 cases in a 25-year period; 54% were male. The incidence of PLA in Danish men was 6 per million in 1977 and 18 per million in 2002. In women, the incidence rose from 8 per million to 12 per million in the same period. Mortality rates in 1977 were 40% and 50% for men and women, respectively, and decreased to a global 10% in 2002.
Clinical Presentation
Liver abscesses may have a broad array of symptoms and physical findings, which may vary according to the patient’s underlying condition. Cryptogenic lesions are often found after several days of nonspecific symptoms. The most frequent clinical features include fever of more than 38° C and chills. Other symptoms that may be present are general malaise and anorexia. Patients may also have abdominal pain, nausea and vomiting, diarrhea, and weight loss. Although more often found with abscesses of biliary origin, jaundice may be an indicator of systemic sepsis response, and septic shock may be a dramatic form of the presentation. There are no significant differences in clinical presentation between single and multiple lesions, although single PLAs are more frequent in the right lobe of the liver. These symptoms may be present from several days up to several weeks before hospital admission (Chou et al, 1997; Seeto & Rockey, 1996). In another group of patients, PLA is a consequence of an underlying pathologic process that may lead to a faster diagnosis. Benign or malignant biliary disease, intraabdominal infections, and abdominal surgery are frequent causes of abscesses, and imaging studies should be systematically carried out to exclude the presence of a PLA in a septic patient.
Finally, some patients may be seen with systemic complications as a result of metastatic septic lesions that originate from a PLA. Although rare, cases of endophtalmitis; meningitis; cellulitis; lung abscess; prostate, kidney, and joint infections; pulmonary embolisms; and even cardiac tamponade due to pericardic effusion have been reported in the literature (Cahill et al, 2000; Vong et al, 2007). Infection by Klebsiella pneumoniae genotype K1 and an underlying condition of immunosuppression resulting from diabetes mellitus and alcoholism may be predisposing factors for these complications (Chen et al, 2006; Fang et al, 2007).
Diagnosis
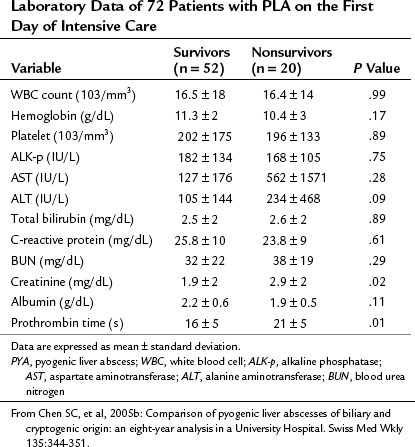
The most common laboratory findings are nonspecific alterations as a result of infection. In a large series from Hong Kong, low albumin levels were found in 92.8% of patients presenting with PLAs (Lok et al, 2008). Leukocytosis (74.8%), increased alkaline phosphatase (72.1%), and elevated alanine aminotransferase levels (ALT; 58.6%) were frequent laboratory abnormalities also present in these patients. Jaundice may be seen in up to 50% of patients, and alkaline phosphatase, gamma-glutamyl transferase, erythrocyte sedimentation rate, and glutamic oxaloacetic transaminase levels are usually elevated (Cosme et al, 2010). Alvarez and colleagues (2001) analyzed laboratory data obtained from patients younger than and older than 60 years. The only significant difference between these two groups was that older patients tended to present with higher blood urea nitrogen and serum creatinine levels. Hemoglobin level, serum C-reactive protein, blood urea nitrogen, creatinine levels, prothrombin time, and total bilirubin levels must be part of systematic laboratory tests in patients with PLA.
Some findings at presentation may be prognostic and associated with increased mortality rate. Chen and colleagues (2008b) presented a review of 72 patients admitted to the intensive care unit. Low levels of serum albumin, increased serum creatinine, and prolonged prothrombin time were significant risk factors for death. These authors’ findings are shown in Table 66.2.
CT has a sensitivity of more than 97% in detecting PLA and is considered the most important imaging modality. Examination should be routinely performed with intravenous contrast enhancement. During the arterial phase, parenchyma surrounding the abscess may show segmental enhancement as a result of altered portal microcirculation in the infected tissue. The typical CT image description of PLA is that of a target-like sign (see Chapter 16) that appears as a single or multiloculated mass with a central hypodense region and peripheral contrast enhancement during the portal phase of examination.
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
 Portal hypertension in children
Portal hypertension in children
 Liver transplantation for cholangiocarcinoma and other neoplastic diseases
Liver transplantation for cholangiocarcinoma and other neoplastic diseases
 Distal splenorenal shunt
Distal splenorenal shunt
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


