Chapter 71 Portal hypertension in children
Special Features of Portal Hypertension in Children
Portal hypertension secondary to chronic liver disease and prehepatic or posthepatic vascular events is a major cause of morbidity and death in both adults and children (see also Chapter 70A). However, children with these conditions provide a different set of challenges in the understanding and management of portal hypertension because of a predominance of congenital etiologies combined with growth and developmental considerations.
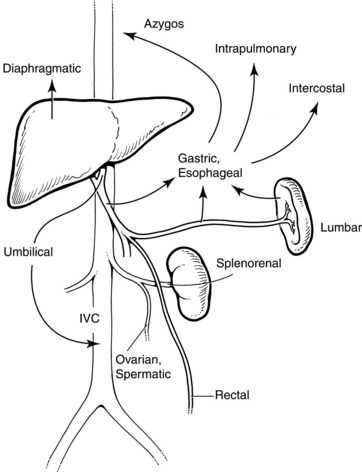
In general, portal hypertension is the result of a combination of increased portal blood flow and increased portal resistance; it occurs when portal blood pressure rises above approximately 10 mm Hg. Signs and symptoms are primarily the result of decompression of this elevated pressure through portosystemic collaterals, but special developmental vascular alterations apply in children (Fig. 71.1). The major problems seen in children are bleeding varices, ascites, and malnutrition. Encephalopathy, portopulmonary hypertension, and hepatorenal syndrome, although important when they do occur, are seen less frequently in children. Splenomegaly and hypersplenism rarely require specific intervention.
Causes of Portal Hypertension in Children
Portal hypertension may arise as a result of an extrahepatic (portal vein), posthepatic (hepatic vein), or intrahepatic block; the block may be presinusoidal, sinusoidal, or postsinusoidal. Causes in children are shown in Box 71.1.
Extrahepatic Causes
Although possibly declining in frequency, extrahepatic portal venous obstruction, caused by a congenital thrombotic or atretic process, is an important cause of noncirrhotic portal hypertension, especially in developing countries but certainly not confined there (Sarin & Agarwal, 2002). Septic or traumatic umbilical vein injury from omphalitis and/or catherization accounts for some cases, but most cases are idiopathic or represent a congenital malformation of the portal venous system. Portal vein stenosis or thrombosis may also occur in the context of portal vein anastomoses in liver transplantation. In the congenital form, the portal vein is transformed into a cavernoma, resulting in portal hypertension and esophagogastic varices. Importantly, from a treatment standpoint, splenic vein or more extensive portal system involvement results in somewhat different hemodynamics, with an extensive collateral circulation involving a preponderance of gastric varices (Shah et al, 2003) and sometimes ectopic varices involving paracholecystic, paracholedochal, and pancreatoduodenal veins. Esophageal bleeding, or sometimes gastric variceal bleeding, is thus the most important consequence, although the presence of naturally occurring shunts may reduce the risk over time, usually by the second decade of life. Besides variceal bleeding, which is the commonest presentation, hypersplenism is common, and anemia, easy bruising from thrombocytopenia, and abdominal pain may be presenting features. Some patients may develop symptomatic portal biliary obstruction. Growth retardation from malabsorption as a result of failure of the enteropancreatic and enterohepatic circulation is not uncommon. Overt encephalopathy as a result of shunting appears uncommon, but subclinical signs may occur, including disturbed neurocognitive function, particularly attention and short-term memory problems (Mack et al, 2006). Although the liver may appear normal, reversible decompensation may be seen after an acute variceal hemorrhage, and functional compromise may develop over the long term.
Intrahepatic Causes
Portal hypertension may result from a range of presinusoidal, sinusoidal, and postsinusoidal causes of increased portal bed resistance within the liver. Presinusoidal conditions, such as congenital hepatic fibrosis, do not result in impaired liver function. Congenital hepatic fibrosis is a developmental disorder that belongs to the family of hepatic ductal plate malformations and is characterized histologically by a variable degree of periportal fibrosis and irregularly shaped proliferating bile ducts (Summerfield et al, 1986). Liver biopsy is highly specific for the diagnosis. In most patients, the first manifestations of the disease are signs or symptoms related to portal hypertension, especially splenomegaly and varices, often with spontaneous gastrointestinal (GI) bleeding that occurs from early childhood and sometimes even into adulthood.
Increased sinusoidal resistance and portal hypertension occur almost invariably in cirrhosis in children. In children, common causes include forms of infant cholestasis, such as biliary atresia, as well as a range of metabolic disorders, infections, toxins, and vascular and nutritional diseases. Cirrhosis is a chronic, diffuse disease characterized by irreversible widespread hepatic fibrosis with regenerative nodule formation (see Chapter 6, Chapter 70A, Chapter 70B ). The prominent fibrous tissue contains vascular anastomoses, which cause hemodynamic alterations and portosystemic shunting. This diffuse pathology superimposed on the primary liver disease often obscures the nature of the original insult. The major pathophysiologic consequences are the result of impaired hepatic function and portal hypertension. Progression to cirrhosis and its complications in pediatric liver diseases is highly variable and represents an important consideration in management, particularly when considering surgical options that may compromise later outcomes. In some conditions, such as neonatal extrahepatic biliary atresia, the development of cirrhosis can be extraordinarily rapid, occurring by 12 to 16 weeks of age with liver failure as early as 24 weeks of age. Early diagnosis and surgical treatment by hepatoportoenterostomy improves outcome, but in most cases, liver transplant becomes the only available treatment option. Other disorders, such as cystic fibrosis–associated focal biliary cirrhosis, can be compatible with normal liver function for many years, presenting with signs of portal hypertension in the second decade of life.
Postsinusoidal intrahepatic conditions, such as venoocclusive disease, are rare in children and usually occur only in the context of chemotherapy for childhood cancers (Gharib et al, 2006) or occasionally related to toxin ingestion, such as from eating poisonous mushrooms. However, posthepatic portal hypertension is a significant condition in children (see Box 71.1). Obstruction to hepatic venous outflow, such as from hepatic vein anastomotic stenosis, can occur after liver transplantation, with Budd-Chiari syndrome, or as a result of cardiac lesions that cause an increase in right atrial pressure and/or chronic systemic venous hypertension. Acute Budd-Chiari syndrome is rare in children; although it may occur with some thrombophilic disorders, it is usually idiopathic and is not associated with the causes seen in adults, such as myeloproliferative disorders. A cavopulmonary or atriopulmonary shunt, known as a Fontan procedure, allows life-saving systemic-pulmonary blood flow in single-ventricle syndromes in neonates but results in chronic systemic venous hypertension (pressures may be >20 mm Hg) and eventually to portal hypertension (Narkewicz et al, 2003).
Effects of Portal Hypertension in Children
The major pathologic effect from portal hypertension is the development of collaterals that carry blood from the portal venous system to the systemic circulation in the upper part of the stomach, esophagus, rectum, and falciform ligament. These collaterals may drain into the IVC via the umbilical vein remnant, or they may drain into the left renal vein (see Fig. 71.1). Absence or disconnection of the IVC or interruption to the azygos system, such as occurs in some cases of bilary atresia, may cause special concern. Similarly, in extrahepatic portal venous malformations, the splenic vein can be small and possibly thrombosed.
Although changes in vascular resistance to flow of blood between the splanchnic bed and the right atrium appear to be the initial events in the development of portal hypertension, a number of other hemodynamic changes contribute to and amplify the increased portal blood pressure. There is a hyperdynamic circulatory state with increased cardiac and decreased splanchnic arteriolar tone, both of which increase portal inflow. Changes in intravascular volume also play an important role, as do alterations in adrenergic tone in the splanchnic system. These observations have led to new experimental and clinical studies that suggest possible pharmacologic treatments for portal hypertension (Boyer, 2001). However, because the major clinical effect is that of bleeding from esophageal varices, direct treatment of variceal hemorrhage, or shunt surgery in selected cases, remains the primary approach, except in the presence of liver decompensation, in which case the treatment of choice is liver transplantation (see Chapters 97A and 98A).
Clinical Features
The main clinical features are splenomegaly, nutritional growth failure, and ascites, along with esophageal, gastric, and rectal varices (Box 71.2).
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Preoperative and postoperative nutrition in hepatobiliary surgery
 Nonhepatic surgery in the cirrhotic patient
Nonhepatic surgery in the cirrhotic patient
 Liver transplantation for cholangiocarcinoma and other neoplastic diseases
Liver transplantation for cholangiocarcinoma and other neoplastic diseases
 Distal splenorenal shunt
Distal splenorenal shunt
 Magnetic resonance imaging of the liver, biliary tract, and pancreas
Magnetic resonance imaging of the liver, biliary tract, and pancreas
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


