Fig. 24.1
The patient is placed in the supine position with legs split
24.5 Access Devices and Instrumentation
RPLS can be performed in many ways using different access devices and specially designed instruments. These devices are generally expensive and cumbersome to use, increasing the cost and prolonging the operative time. However, these shortcomings can be overcome with the single-incision multi-puncture technique. A curvilinear 2.5-cm incision is made around the umbilicus and deepened up to the fascia. The area surrounding the fascia is cleaned by blunt and sharp dissection. A Veress needle is inserted through the fascia into the peritoneal cavity, and a pneumoperitoneum of 12 mmHg is created using carbon dioxide gas. One 10-mm and two 5-mm ports are inserted through the fascia, making multiple punctures via the same incision and maintaining 1 cm distance between these ports. If needed, a 0.5-cm slit on either side of the curvilinear incision can be made to achieve this 1-cm distance between the trocars. This arrangement provides a narrow triangulation for the working instruments, facilitating intracorporeal suturing, a vital prerequisite for this procedure (Fig. 24.2). The 10-mm port is placed first in the center of the incision, and one 5-mm port is placed on each side at 2 o’clock and 10 o’clock. Furthermore, to reduce the clashing of instruments, two modifications are incorporated. First, instruments of different lengths are used for both hands which makes them to work at different distances from the abdomen. Second, a long telescope with a co-axial light cable is used to further reduce the crowding and clashing (Fig. 24.3). Using an endostapler, the 10-mm port is changed to a 12-mm, and a 5-mm scope is used briefly. No extra ports (or needlescopic ports) are needed for this procedure.

Fig. 24.2
Achieving narrow triangulation in single-incision multiport technique
Fig. 24.3
Instruments of different lengths with a long telescope with a co-axial light cable is used to further reduce the crowding and clashing
24.6 Retraction of Tissues
The retraction of tissues is a contentious issue in RPLS. Apart from the liberal use of gravity, there are many methods for retracting the stomach and liver. Liver retraction is usually not required during LPJ, but in the case of a large left lateral segment, sometimes it is necessary to retract the liver. We fix a piece of corrugated drain to sutures at both ends to lift up the liver. Retraction of the stomach, on the other hand, is critical to expose the entire length of pancreas. This is done using retracting sutures placed in the posterior wall of the stomach close to the greater curvature. The suture ends are then brought out through a suture passer. This arrangement hooks the stomach to the anterior abdominal wall (Fig. 24.4).
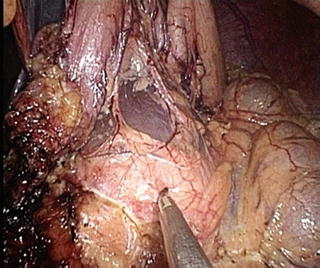
Fig. 24.4
Stomach hooked to anterior abdominal wall
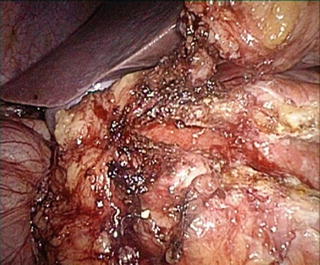
24.7 Operative Technique
The lesser sac is entered by dividing the gastrocolic omentum using ultrasonic shears, and the stomach is separated from the pancreas. The stomach is retracted as previously described. The pancreas is exposed completely after dividing the right gastroepiploic vessels. The duct is then opened from head to tail using ultrasonic shears. The location of the pancreatic duct is confirmed using needle aspiration or, in difficult situations, an intra-operative ultrasound probe. Intraductal stones are cleared completely along the entire length of the duct (Fig. 24.5). Care must be taken to open the duct in the head region, a process that requires safe parenchymal division to avoid bleeding. From our experience in laparoscopic surgery, we have learnt that the most common complication during the procedure is bleeding from the edge of duct opening. If branches from the gastroduodenal arcade are damaged, they can be suture ligated, as using cautery alone may be insufficient. Ultrasonic shears are best to open the duct. The entire procedure is similar to already prevalent techniques for LPJ, except for the type of access and stomach elevation. The single-incision technique requires no compromise, and the entire dissection is performed under clear display of the surgical field.