Fig. 32.1
The single trocar device (SILSTM port (Covidien)) is introduced in place
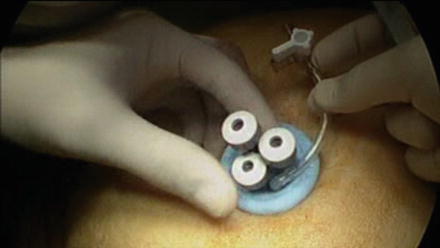
Fig. 32.2
The SILSTM port (Covidien) is used with three 5-mm working channels: one for a roticulator grasper in the left hand of the surgeon, one for the 5-mm optic and the last one to introduce different standard laparoscopic straight instruments, such as the endoscopic graspers, and the endoscopic scissors and dissectors with electrocautery. The abdominal cavity is insufflated up to 14 mmHg of pressure through the port device
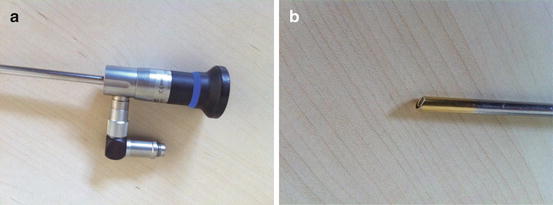
Fig. 32.3
(a, b) 5-mm 30º scope with the angle for the light source
At this stage, we place the patient 10–15° head down. The principles of TAPP repairs are the same and must be followed to avoid injuries to bladder, vessels, nerves, and vas deferens. The maneuvers to identify the anatomical structures of the area and to dissect of the hernia sac are performed with a flexible grasper (Roticulator Endodissect/grasp (Covidien)) in the left hand, through one of the 5-mm orifice, using the other 5-mm orifice to introduce different conventional straight instruments, such as the endoscopic graspers, scissors and dissector with electrocautery. We consider that this combination of instruments avoids surgery with surgeon’s hands crossed, thus decreasing the consequent learning curve of this procedure. The dissection proceeds then just the same as for conventional endoscopic TAPP repair: a flap of the peritoneum is created with the endoscopic scissor 2-cm above the superior edge of the hernia (Figs. 32.4 and 32.5), the symphysis pubis is identified and dissected free of areolar tissues and the bladder, the inferior epigastric vessels are then identified, and the lateral space is then dissected and continued medially until the cord structures are identified. An indirect sac and its accompanying lipoma of the cord are reduced with sufficient proximal dissection of the peritoneal reflection to allow the inferior edge of the mesh to lie well clear of it. This dissection then continues medially and any direct sac is reduced.
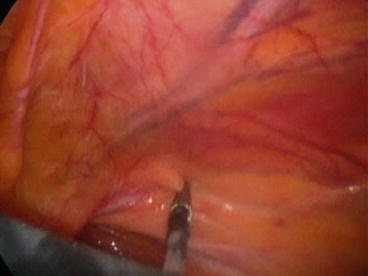
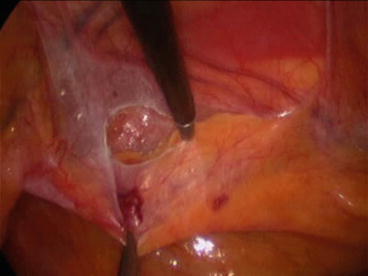
Fig. 32.4
The roticulater grasper grasps the perito-neum 2-cm above the superior edge of the hernia
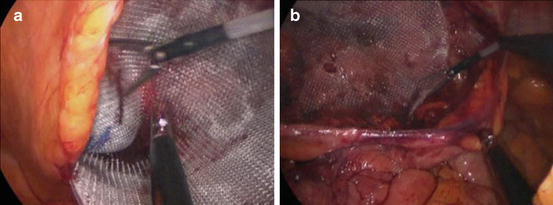
Fig. 32.5
A flap of the peritoneum is created with the endoscopic scissors with electrocautery
Once the sac is reduced, one of the 5-mm ports is replaced for a 12-mm port in the device in order to introduce the mesh, replacing the 5-mm port to continue the surgery. An anatomical pre-shaped mesh (3DMax Mesh®, Bard Davol Inc., Warwick RI, USA) is introduced through the 10–12 mm orifice of the SP devices and placed covering all the weak areas of the inguinal region (Fig. 32.6a, b). The mesh is correctly expanded. Although the mesh could be left in place without any fixation, fibrin glue (Tissucol®, Baxter, Vienna, Austria) is used in most of the cases, avoiding mechanical fixation in order to decrease postoperative pain. The peritoneal flap is closed, avoiding the mesh being exposed to the bowel (Fig. 32.7), using a conventional running suture, tacks or new closure devices, such us V-loc® (Covidien). This last new device is a revolutionary technology that eliminates the need to tie knots, so the incision can be closed up to 50 % faster without compromising strength and security. Finally, the fascia is closed with interrupted sutures and the skin is also closed.