Fig. 39.1
A view of minimally invasive surgery integrated operating theatres in our institution
39.2.1 Instruments/Equipment
There is a large range of products available for the surgeon to utilize. Flexible, articulated, or pre-bent instruments are generally recommended to help achieve triangulation during surgical procedures. A combination of both straight and articulated or pre-bent instruments may facilitate the maneuvers and reduce conflict among instruments. It important to choose an appropriate telescope to reduce clashing; in our experience, the EndoEYE 5-mm 30° (Olympus) is one of the most comfortable options. Other alternatives include a long 10-mm 30° telescope similar to the one used in bariatric surgery, or a telescope with a flexible tip (EndoEYE Flex HD (Olympus)). For advanced procedures and when required, the use of energy-sealing devices is recommended. Today, there are several devices using different types of energy for sealing and cutting vessels up to 7-mm, ranging from ultrasonic waves to HF bipolar diathermy, or even a combination of both. By using an energy-sealing device, tissue can be dissected and transected with minimal traction as compared to using conventional diathermy. Lastly, percutaneous suture for retraction can be a useful strategy to improve retraction and surgical exposure. One or two percutaneous non-absorbable sutures can offer additional benefits when a reduced number of ports affects the technique (Fig. 39.2a, b).
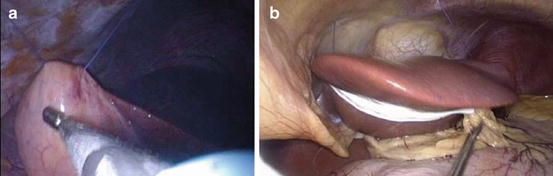
Fig. 39.2
(a, b) Two different utilizations of percutaneous suture for organ retraction
39.2.2 Port Placement
Prior to placing the port, thought should be given to the target pathology with regards to the working area within the abdomen. Many procedures can be performed via a single peri-umbilical port. For example, a left trans-peritoneal adrenalectomy and cholecystectomy are feasible if performed via a peri-umbilical port, whereas a ventral peri-umbilical hernia repair with an ovarian cystectomy would require the port being placed in the lower quadrant or flanks (Fig. 39.3a, b).
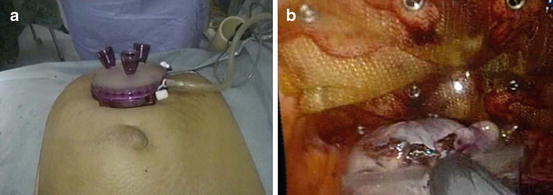
Fig. 39.3
(a, b) Port position and intraoperative view of SPES ventral hernia repair and oophorectomy
Adjustment of the port may be required in certain situations. For example, a totally extra-peritoneal inguinal hernia repair can be first performed extra-peritoneally, with the port being placed first in the pre-peritoneal space, and adjustments being made later to advance it intra-peritoneally for the second procedure, such as cholecystectomy.
39.3 Tips and Tricks (Compared to Multi Trocar Laparoscopy)
It is paramount to understand that there is no standard technique when performing RPLS or SPES for multiple procedures. A certain degree of creativity is required to accommodate the multitude of procedures.
Proper port placement is the corner stone for this technique, as improper port placement would result in almost certain conversion to conventional laparoscopic techniques/open surgery.
Proper thought into which procedure should be performed first is important as well. It would be logical to perform the more medically pressing procedure first. Should major difficulties arise with the first procedure, postponement of the second procedure can be considered.
There should be no hesitation to revert to conventional laparoscopic surgery or to insert additional ports should the need arise, as patient safety is paramount.
39.4 Recommendations from the Author
RPLS or SPES for two or combined procedures is only for advanced laparoscopic surgeons who have surmounted the learning curve in SPES.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


