Chapter 58B Pancreatic cancer
Clinical aspects, assessment, and management
Clinical Presentation
Ongoing research has produced a multitude of potential biomarkers for pancreatic cancer (Harsha et al, 2009). The only biomarker that has recognized clinical utility is carbohydrate antigen 19-9 (CA19-9); however, its usefulness has two significant limitations. First, it is not specific for pancreatic cancer because it can be elevated in benign conditions, particularly those that cause obstructive jaundice. Second, its sensitivity is reduced by the fact that patients who test negative for Lewis blood group antigens A and B are unable to synthesize CA19-9 and therefore do not express it in their serum. The percentage of pancreatic cancer patients who fall into this group has been reported to range from 10% to 34% (Berger et al, 2008; Tempero et al, 1987). Thus CA19-9 best serves as a marker of treatment response and recurrence in patients who have a pathologic diagnosis of pancreatic cancer.
Diagnosis
Once suspicion is sufficient for pancreatic cancer, high-quality imaging is critical for diagnosis and treatment planning. Many patients initially undergo an abdominal ultrasound (US) or a limited computed tomography (CT) scan of the abdomen. These modalities will suggest processes in the pancreas that require appropriate evaluation. Currently, the best diagnostic modality for imaging the pancreas is a pancreas protocol multidetector CT with dedicated arterial and venous phases and three-dimensional (3D) reconstruction (see Chapter 16; Buchs et al, 2010; Horton & Fishman, 2002). Water is given orally, and contrast is given intravenously. Such scans typically demonstrate the tumor as a low-density (hypodense) lesion within the pancreas, best seen during the venous phase of contrast enhancement. Importantly, these high-quality imaging studies show the important relationship between the tumor and the surrounding visceral vessels, including the superior mesenteric vein, portal vein, splenic vein, superior mesenteric artery (SMA), and the branches of the celiac axis. Such high-quality CT imaging can reliably predict visceral vessel involvement, and thereby surgical respectability, approximately 80% to 90% of the time (House et al, 2004; Karmazanovsky et al, 2005). Additionally, the arterial phase with 3D reconstruction can assist in surgical planning by identifying variations in hepatic arterial anatomy and other vascular anomalies preoperatively, most notably a “replaced” right hepatic artery originating from the SMA, which is seen in one of six patients (see Chapter 1B).
Continuing improvement in the technology that produces magnetic resonance imaging (MRI) has resulted in image quality and resultant diagnostic sensitivities that approach those of CT (see Chapter 17). A recent meta-analysis of 68 articles calculated an overall diagnostic sensitivity of 91% for CT, compared with 84% for MRI, and reported diagnostic specificities of 85% and 82%, respectively (Bipat et al, 2005). Regarding determination of resectability, CT had a sensitivity and specificity of 81% and 82% compared with MRI at 82% and 78%, respectively. No advantage has been demonstrated by obtaining both CT and MRI for uncomplicated patients who display classic symptoms of pancreatic cancer, and this practice should be discouraged. We typically reserve the use of MRI for patients with renal impairment or sensitivity to the intravenous contrast used for CT. The use of MR cholangiopancreatography (MRCP) is valuable in evaluating and following small cystic lesions of the pancreas, but a detailed discussion of these lesions is outside the scope of this chapter (see Chapters 17 and 57).
Endoscopic evaluation of patients with classic symptoms of pancreatic cancer is appropriate in specific situations. Esophagogastroduodenoscopy (EGD) is appropriate in cases of gastric outlet obstruction to assess the anatomy and presence of other diagnoses. In the presence of metastatic or unresectable disease, or when a patient is not physiologically appropriate for immediate surgical intervention, a therapeutic EGD combined with duodenal stenting can be of some benefit, allowing the patient to return to oral intake (see Chapter 27). Endoscopic retrograde cholangiopancreatography (ERCP) was once commonly used as a diagnostic modality for patients with a suspected periampullary pancreatic cancer. With the improvement of cross-sectional imaging, the use of strictly diagnostic ERCP is currently unsupported. Therapeutic ERCP with stenting of biliary strictures can be of benefit in the same patient population (metastatic, unresectable, or physiologically unfit) as therapeutic EGD (see Chapters 14, 18, and 27). However, the routine placement of a biliary endoprosthesis for all patients seen with jaundice without cholangitis should be discouraged. Multiple studies have shown a doubling of the wound infection risk and a slight increase in overall complication risk with preoperative biliary stenting (Pisters et al, 2001a; Sohn et al, 2000). For most patients seen initially with a pancreatic mass and jaundice, early surgery is preferable to endoscopic stenting and delayed surgical resection (Kennedy et al, 2010).
Endoscopic ultrasound (EUS) is a relatively new imaging and diagnostic technology compared with those previously discussed (see Chapter 14). Well established at specialty referral centers, it is rapidly becoming more widely available. Interpretation of EUS imaging is operator dependent, a factor that may account for the wide range of diagnostic sensitivities reported in the literature and encountered in real-world clinical settings (Ahmad et al, 2000; Gress et al, 1999; Hunt & Faigel, 2002; Palazzo et al, 1993; Rösch et al, 1991; Varadarajulu & Eloubeidi, 2010). Reported sensitivities for the diagnosis of pancreatic neoplasia have ranged from 69% to 94%. Several studies have found EUS to be superior to CT for the detection of lesions smaller than 2 cm. EUS is of particular utility when a patient has a presentation consistent with pancreatic cancer (biliary or pancreatic duct obstruction) but no evidence of mass on cross-sectional imaging. The ability of EUS to accurately estimate T-stage decreases compared with CT for larger lesions. Additionally, EUS has shown some superiority over CT for the detection of venous invasion, but it is less useful for the determination of arterial involvement (Varadarajulu & Eloubeidi, 2010). An important additional advantage of EUS is the ability to obtain tissue via fine needle aspiration (FNA) for diagnostic purposes at the time of evaluation. This can be of great benefit to unresectable or marginally resectable patients who need a confirmed tissue diagnosis prior to the initiation of chemotherapy. However, for the vast majority of patients with a symptomatic pancreatic mass that appears completely resectable by CT or MR imaging, EUS with FNA is not needed; in most cases the mass will require resection regardless of the EUS and FNA results.
18Fluorodeoxyglucose-positron emission tomography (18FDG-PET) is a functional imaging modality based on the observation that neoplastic cells exhibit accelerated glucose uptake and metabolism (see Chapter 15). Once transported into the cell and phosphorylated by hexokinase, the first step in glycolysis, 18FDG remains trapped within the cell. Although studies suggest 18FDG-PET is sensitive for the detection of pancreatic cancer, the precise role of this technique in the diagnosis and staging of patients with localized pancreatic cancer is limited. Its use is confounded by the difficulty 18FDG-PET has in distinguishing benign from malignant masses as a result of localization, both to sites of inflammation and infection and to neoplasms. 18FDG-PET is of greater utility in evaluating indeterminate masses in the liver that are not amenable to biopsy. A tissue diagnosis of a primary mass made by EUS, when combined with a PET-positive liver lesion, is adequate to initiate palliative chemotherapy at many centers.
Staging
Pancreatic cancer is staged by the seventh edition (2010) of the American Joint Committee on Cancer (AJCC) Cancer Staging Manual, according to clinical parameters that are available from high-quality CT imaging (Edge, 2010). Classic T, N, and M parameters are used for tumor size, nodal involvement, and distant metastases, but stage grouping is performed according to resectability. Patients are classified as having localized resectable disease (stages I and II), locally advanced unresectable disease (stage III), or distant metastatic disease (stage IV; Table 58B.1). A resectable tumor is characterized on CT by no evidence of metastatic disease, a clear tissue (fat) plane between the tumor and the visceral arteries (celiac axis and SMA), and 180-degree or less circumferential involvement of the superior mesenteric vein–portal vein confluence (Fig. 58B.1). In contrast, patients with unresectable disease exhibit distant metastases, ascites, or involvement of the celiac axis or SMA (Fig. 58B.2). Venous vascular involvement is considered potentially resectable in the AJCC system and is therefore categorized as stage II disease, and arterial involvement is considered unresectable and is categorized as stage III disease. A small subset of patients with complete occlusion of the superior mesenteric vein–portal vein confluence and significant collateralization that precludes safe venous resection and reconstruction are typically deemed unresectable but are still classified as stage II in the current AJCC system. This system has been validated by correlation to overall survival (OS) using the National Cancer Database (Table 58B.2; Bilimoria et al, 2007a).
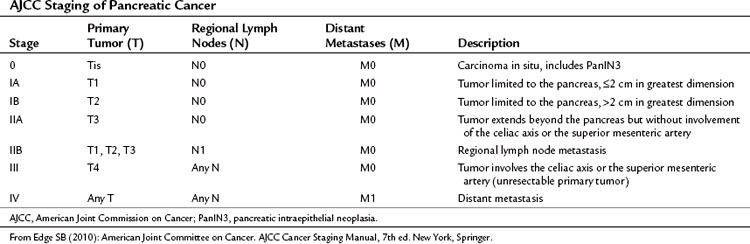
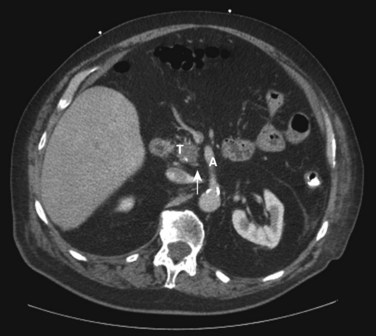
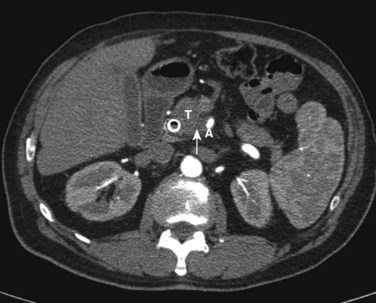
FIGURE 58B.2 Unresectable pancreatic adenocarcinoma in the head and uncinate process, showing loss of fat plane (arrow
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
 Portal hypertension in children
Portal hypertension in children
 Liver transplantation for cholangiocarcinoma and other neoplastic diseases
Liver transplantation for cholangiocarcinoma and other neoplastic diseases
 Distal splenorenal shunt
Distal splenorenal shunt
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


