Fig. 1
Seminoma. Sonogram demonstrates a minimally heterogeneous, well-marginated intratesticular mass
Staging involves clinical, pathologic, radiologic, and serum-tumor-marker data [1]. In broad categories, tumors limited to the testis are stage I, those with retroperitoneal nodal involvement are stage II, and those with distant disease are stage III [1]. Nodal disease is usually initially assessed with computed tomography (CT), although MRI has assumed a greater role in recent years in view of concerns regarding radiation exposure in this group of men who are typically between 20 and 40 years of age at the time of diagnosis. This is especially relevant for follow-up in patients with seminoma who not only have a generally favorable prognosis (including response to salvage regimens when needed) but also are frequently offered observation rather than prophylactic therapeutic radiation [5]. Fluorodeoxyglucose positron emission tomography (FDG PET) is not presently included in the initial staging of testicular malignancy due to a lack of evidence to support its routine use [1, 6]. Results have been somewhat mixed, however, in the setting of followup after initial treatment; FDG PET may have a role in certain patients (especially those with nonspecific findings when evaluating for active tumor, specifically for seminoma patients being followed to assess response after chemotherapy) [5].
Regardless of stage, nearly all patients with suspected testicular neoplasm are managed surgically (orchiectomy), which is intended to not only provide pathologic confirmation but also to treat the primary tumor. In patients who, based on age (e.g., <30) and imaging features (e.g., heterogeneity or calcification) have a higher likelihood of NSGCT, preorchiectomy CT may warrant consideration, as some clinicians will consider contemporaneous retroperitoneal lymph node dissection if the CT is negative for pathologically enlarged nodes (enlarged nodes, >8 mm, are presumptive evidence of stage II disease). Because most surgeons will await final pathologic confirmation before determining management, the differentiation of NSGCT vs seminoma is rarely of critical importance.
Testicular Microlithiasis
The topic of testicular microlithiasis (TML) has been the source of considerable controversy in the imaging and urologic communities over the past 20 years [7, 8]. There is little debate that TML, when defined as at least five calcifications in a single sonographic field (Fig. 2), is associated with both intratubular germ-cell neoplasia (a malignant precursor) [9] and an empirically demonstrated increased risk of malignant GCT. Some authors point to a lack of a significant associated risk but often fail to recognize that accepting a very broad definition of TML (e.g., any isolated calcification) incorrectly defines a very large population, which dilutes the importance of the disease by decreasing the specificity of the finding. Many radiologists continue to recommend sonographic follow-up for patients with convincing evidence for TML, especially in younger individuals (e.g., <40 years) [10].
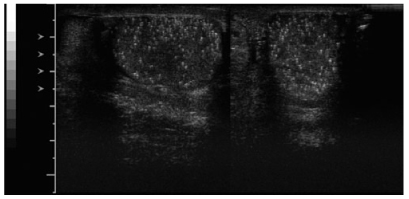
Fig. 2
Testicular microlithiasis. Innumerable echogenic foci in both testes
Gonadal Stromal Tumors
Gonadal stromal tumors (GST) account for <10% of testicular neoplasms and include Leydig cell and Sertoli tumors. These are often incidental findings although may cause gynecomastia. For practical purposes, they are almost always benign but are surgically removed to confirm the diagnosis; imaging and clinical features do not allow differentiation from the more common malignant GCT mentioned above [3].
Lymphoma
Lymphoma is usually seen in older patients than those affected by GCT. More importantly, almost all patients with testicular lymphoma have known disease prior to the development of scrotal signs or symptoms. The epididymis may be affected, but testis involvement is more common. Whereas the appearance may overlap with that of GCT, lymphoma is more likely to be multifocal or even bilateral [3]. Conspicuous hypervascularity on Doppler US imaging compared with the more common primary neoplasms has been described. It is difficult to differentiate lymphomatous from leukemic involvement of the testis, although, as noted above, the diagnosis is usually known before the patient presents for scrotal imaging.
Extratesticular Neoplasms
Extratesticular neoplasms in adults are uncommon. The two most common lesions are lipomas and adenomatoid tumors. Lipomas are rarely a clinical or imaging challenge to diagnose. Adenomatoid tumors are well-marginated, benign, solid masses that may be ignored when small but may be removed if large enough to cause pain or if there is concern regarding the diagnosis [11].
Mesothelioma
Mesothelioma is a rare but aggressive scrotal neoplasm that arises from the tunica. It is far more likely to arise from the pleura or peritoneum than the scrotum and is typically a locally advanced process at the time of initial presentation. Hydrocele or hematocele is commonly seen, and soft tissue nodules of the tunica may be surrounded by fluid. Whereas findings are nonspecific and may mimic unusual soft tissue malignancies, such as leiomyosarcoma, imaging and clinical findings will mitigate for surgical diagnosis and treatment [11].
Papillary Cystadenomas
Papillary cystadenomas of the epididymis are extremely rare but may be seen in 20–25% of patients with von Hippel-Lindau disease. The lesions are benign, solid, well-marginated, and may be difficult to differentiate from the more common adenomatoid tumors.
Tubular Ectasia
Tubular ectasia is not neoplastic but may be mistaken for a mass lesion. The finding is the result of dilatation of the rete testis, with elongated, anechoic channels that converge to the epididymis. Etiology in most cases is uncertain, although obstructive pathophysiology (e.g., postvasectomy) is associated. A nonspherical linear process with angulated margins and, usually, distinct anechoic channels will allow for confident diagnosis. When sonographic findings are atypical, MRI will allow confirmation by demonstrating a well-marginated T2-hyperintense focus [12].
Related posts:
 Enterography: Small Bowel Imaging That Impacts Patient Management
Enterography: Small Bowel Imaging That Impacts Patient Management
 to Perform and Report Magnetic Resonance Imaging for Pelvic Floor Dysfunction: An Interactive Case-Based Approach
to Perform and Report Magnetic Resonance Imaging for Pelvic Floor Dysfunction: An Interactive Case-Based Approach
 Should it Be Integrated into Screening and Clinical Routine Imaging?
Should it Be Integrated into Screening and Clinical Routine Imaging?
 in Hepatobiliary-Pancreatic Tumors
in Hepatobiliary-Pancreatic Tumors
 Abdominal Disease: Diagnosis and Therapy
Abdominal Disease: Diagnosis and Therapy
 Urography in Children
Urography in Children
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


