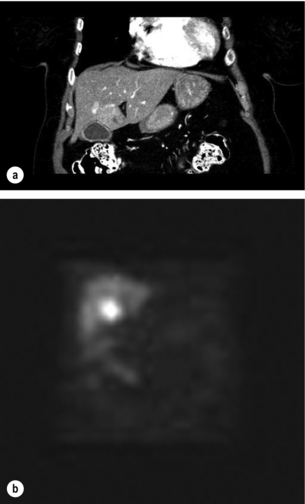
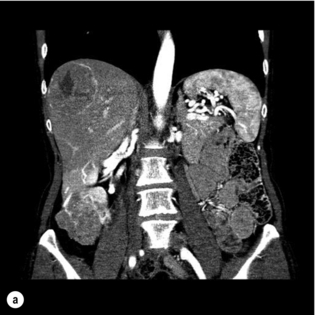
7 The development of liver metastases was previously considered a preterminal event with treatment limited to palliation; however, the success of hepatectomy in improving outcomes in metastatic CRC has generated renewed enthusiasm in considering resection of liver metastases from non-colorectal primary cancers. Liver resection has become the standard of care for CRC liver metastases and many centres have adopted an increasingly aggressive approach, with reported 5-year survival rates exceeding 50%.1,2 The complementary use of portal vein embolisation, radiofrequency ablation and staged resection strategies has increased the proportion of patients eligible for resection. At the same time, advances in surgical technique and knowledge of liver anatomy have reduced significantly the morbidity and mortality associated with liver resection to less than 20% and 5%, respectively.2,3 Liver metastases of non-colorectal origin constitute a diverse group of tumours, most commonly arising from gastrointestinal sites. These tumours can be broadly divided into neuroendocrine and non-neuroendocrine malignancies, encompassing unique and markedly varied natural histories. Neuroendocrine tumours (NETs) have historically been described as indolent malignancies with hepatectomy for NET liver metastases associated with 5- and 10-year survival rates of 77.4% and 50.4%, respectively.4 While hepatectomy is an increasingly accepted management strategy for NETs, it is performed less frequently for non-neuroendocrine tumours. The evidence regarding hepatectomy for non-colorectal metastases originates largely from retrospective reviews spanning several decades of experience.5–8 Many studies fail to distinguish between NET and non-NET metastases, and when that distinction is made, the non-NET metastases are usually considered a single entity despite comprising a heterogeneous set of pathologies. Reports focusing on a single tumour type are usually based on small case series. With advances in surgical techniques and promising results observed in CRC and NET hepatic metastases, the role of surgical treatments in non-NET liver tumours has once again become an area of active research. Due to the paucity of prospective, controlled data, the appropriate indications for hepatectomy for non-CRC metastases are unclear. Factors routinely associated with improved long-term outcomes include a long disease-free interval between treatment of the primary tumour and development of liver metastasis, little or no extrahepatic disease, the projected future liver remnant and well to moderately differentiated cancer.9 The inability to resect all NET liver metastases does not appear to worsen overall survival.4 Unfortunately, no single measure of tumour biology yet exists. The rationale behind a surgical approach to metastatic disease is based on the concept of site-specific metastases. First proposed by Paget in 1889, this ‘seed and soil’ hypothesis argues that solid tumours have a distinct pattern of distant organ involvement created by the target organ microenvironment. Ewing proposed a ‘mechanical’ theory in which the metastatic pattern is determined by the venous drainage of the primary tumour.10 Neither theory takes into account the complexity of the metastatic process, which requires that a cancer cell gains specific invasion and metastatic potential before it can disseminate. The clonal selection model of the metastatic process suggests that heterogeneity develops within a population of cancer cells through mutational events, allowing a subpopulation to randomly acquire the necessary traits to disseminate successfully.11 Alternatively, it has been argued that within cancers of the same pathological type, i.e. breast cancer, some tumours are a priori more likely to develop metastases than others. This is supported by gene expression data where specific molecular signatures have been found to predict accurately prognosis in breast cancer,12 ovarian cancer13 and melanoma.14 Similarly, in CRC the genotype of microsatellite instability correlates with a decreased likelihood of metastatic spread.15 A recent refinement to Paget’s hypothesis, based on molecular genetic research, suggests that the primary tumour is itself capable of preparing the soil by creating a ‘premetastatic niche’.16 Every cancer has a type-specific pattern of cytokine expression that appears to direct both malignant and non-malignant cells to specific distant organs. The influx and clustering of bone-marrow-derived haematopoietic cells is one of the earliest events in the development of a metastatic deposit. This is closely followed by local inflammation and the release of matrix metalloproteinases. These local events appear to mediate remodelling of the extracellular matrix, creating a more permissive microenvironment for the eventual deposition and growth of malignant cells.17 Thus, the primary tumour both chooses and alters the sites to which it metastasises. For reasons not yet understood, many solid tumours metastasise preferentially to the liver. If the site-specific hypothesis of metastatic spread is correct, complete surgical excision of liver metastases can remove the only site of disease and offers a chance for cure. Nonetheless, residual micrometastatic disease may exist within the liver, and hepatic recurrences are a common cause of treatment failure following hepatectomy. Even in the presence of micrometastases, the removal of all macroscopic disease may have immunological benefits. The immune-suppressing effects of cancers are well accepted: malignant cells can induce both adaptive and innate immune suppression, facilitating tumour growth.18 The degree of immune suppression correlates with the tumour burden19 and if all gross metastatic disease can be removed, host defences may attack micrometastatic deposits more effectively. The use of neoadjuvant or adjuvant chemotherapy may improve cure rates by controlling micrometastases.20,21 The advent of next generation sequencing technologies and high-density oligonucleotide arrays has further deepened our understanding of the metastatic process. Whereas the ability of a cancerous cell to metastasise was once believed to occur following the accumulation of multiple somatic mutations in many cancer-causing genes, new findings, specifically in pancreatic cancer, have challenged this belief. Studies by Yachida et al.22 and Campbell et al.23 describe the existence of multiple subclones within a primary pancreas cancer tumour, each containing a unique genetic signature corresponding to an eventual site of metastastic spread. These subclones are present many years before an eventual metastasis is clinically detected, when disease is at an early stage. Furthermore, metastases seen in different organs share many common genetic mutations as well as site-specific changes that confer a selective growth advantage in the respective tissue. Future studies on the biology of metastases are likely to improve our understanding of this complex process, translating into more efficacious therapy. Some patients can be assessed for recurrence using more targeted techniques and biochemical markers (i.e. CA-125 for ovarian cancer, chromogranin A for NETs). Nuclear imaging can detect NETs expressing somatostatin receptors with 80–90% sensitivity. Whole-body PET scanning using a new somatostatin analogue, [68Ga]DOTA-TOC, has been found to be accurate for the detection of new metastases in NETs following radionuclide therapy.24 Occasionally, the original presentation of an NET will be a liver metastasis from an unidentified primary, and the investigative focus is aimed at localisation of the primary tumour. Certain tumours, such as gastric, breast and ovarian cancer, have a predilection for intraperitoneal spread. Although CT is the preferred modality for diagnosing peritoneal carcinomatosis, its accuracy is still limited by histological type, the anatomical site of spread and the size of tumour deposits.25 For many of these equivocal cases, diagnostic laparoscopy has been recommended. Routine laparoscopy with laparoscopic ultrasound for patients with potentially resectable non-colorectal liver metastases has been found to result in a change in management in 20% of cases and may be used in preoperative staging.26 Several treatment modalities exist for metastatic disease, and the therapeutic approach must be tailored to the tumour type, the performance status of the patient and the extent of disease, determined in the setting of a multidisciplinary conference. Ablative strategies and systemic or locally delivered chemotherapy can be used as adjuncts to resection. Radiofrequency ablation (RFA) has been reported to be safe and successful at achieving local control in patients with liver metastases from breast cancer,27 ovarian cancer28 and NETs,29 but its major limitation is the difficulty of achieving complete necrosis for tumours larger than 3 cm. Transarterial embolisation (TAE) takes advantage of the differential blood supply of liver metastases, which depend mainly on the hepatic arteries, and the normal parenchyma, which relies more heavily on the portal vein. Transarterial chemoembolisation (TACE) involves the local delivery of a drug prior to occluding the artery and allows prolonged exposure of the tumour to the agent without increasing systemic toxicity. Both TAE and TACE have been well described for the treatment of unresectable hepatocellular carcinoma30 and the symptomatic relief of NETs.31 Most NETs of gastrointestinal origin demonstrate ‘indolent’ growth. Despite such a benign description, 46–93% of patients with NETs will have liver involvement at the time of diagnosis, with 5-year untreated survival of 0–20%.32 Systemic chemotherapy with platinum-based regimens has shown a response rate of up to 67% in poorly differentiated NETs. Nevertheless, the survival benefit of chemotherapy is limited and associated with significant toxicity.33 Somatostatin analogues such as octreotide can achieve symptomatic relief in 70–80% of patients, but an antiproliferative effect is seen in less than 10% of cases.34 Furthermore, newer agents such as the receptor tyrosine kinase inhibitor sunitinib, the mammmalian target of rapamycin (mTOR) inhibitor everolimus, and the anti-vascular endothelial growth factor (anti-VEGF) bevacizumab have shown promise in PNETs.33 NETs metastasise preferentially to the liver, and in many patients the liver remains the only site of metastatic disease for a prolonged period of time. The majority of patients have multifocal, bilobar disease, of which less than 20% are candidates for surgery32 (Fig. 7.1a,b). Liver resection may be performed with curative intent, symptom control or prolongation of survival in the palliative setting. Figure 7.1 (a) A 67-year-old female with a node-positive distal jejunal carcinoid tumour and synchronous solitary liver metastasis in segment 4B. (b) Octreotide scan of the same patient. Transaxial single-photon emission computed tomography (SPECT) demonstrates abnormal activity in segment 4B corresponding to known metastasis on CT. The choice of treatment for NET hepatic metastases is largely dependent on underlying tumour biology and pattern of metastatic spread.35 According to the 2010 World Health Organization guidelines for the management of NETs, pathological grade (1-3) has been highlighted as an important marker for underlying tumour biology affecting survival.36 Pathologic grade is determined microscopically by the number of cellular mitoses per high powered field (hpf) and through Ki-67 labelling of tumours. NETs with <2mitoses/10hpf and <3% Ki-67 index are classified as low grade (G1) well-differentiated tumours whereas NETs with >20/10hpf and >20% Ki-67 labelling are denoted as high grade (G3) and poorly differentiated. Recent studies have shown that G3 NETs exhibit a poor prognosis following surgical management for hepatic metastases and are better treated non-operatively with chemotherapy.36 The metastatic pattern of spread in the liver for NETs also has prognostic implications and is categorized into three morphological subtypes:35,36 (I) “restricted metastases” involving one lobe or two adjacent segments; (II) “dominant lesion with bilobar metastases” whereby a single major focus is accompanied by multiple contralateral satellite lesions; (III) diffuse, multifocal liver metastases affecting multiple segments within and between lobes. Patients with Type I or II (25% and 15% of cases respectively) disease, in the absence of metastases at distant extrahepatic sites are considered for curative surgical resection.35,36 The aim of liver resection with curative intent in NETs is to leave no residual disease (R0 resection) in both primary and secondary sites, and this may be associated with 5-year survival rates of up to 85%.31,32 Surgical indications include the presence of a resectable well-differentiated NET without extra-abdominal metastases or peritoneal carcinomatosis, in a patient without right-sided cardiac dysfunction.35 Optimal cytoreduction aims to reduce tumour volume by at least 90%.32 Although there are no data from randomised trials, large series using historical controls or contemporary cases matched for stage have demonstrated that liver resection with optimal cytoreduction results in improved survival.37–39 Hepatic resection for metastatic NETs results in improved overall survival compared to those receiving supportive care. Furthermore, R1 and R2 resections result in 5-year survival rates of 70% and 60%, respectively,32 challenging the dogma that surgery should be reserved only for patients most likely to have an R0 resection. Cytoreduction similarly offers the most effective and durable palliation from symptoms.38,40 As a result, surgical debulking has been advocated for both functional and non-functional tumours.41 An aggressive approach, sometimes combining liver resection with other ablative strategies, is warranted (Fig. 7.2a,b). Figure 7.2 (a) A 59-year-old female with an incidental finding of multiple NET metastases. There was no evidence of primary tumour on octreotide scan and endoscopy. Note multiple hypervascular, large metastases with central necrosis. (b) Same patient as in (a). A debulking operation to remove 90% of tumour burden would be possible by performing an extended right hepatic lobectomy with wedge resections from segment 2. Most series of hepatic resection for metastatic NETs include an occasional case with an unknown primary, despite thorough imaging and endoscopy. Although survival data are sparse, an aggressive resectional approach for these patients is reasonable (Fig. 7.2b). Non-surgical treatment modalities include RFA, TAE and TACE. RFA in isolation can achieve symptomatic relief and local control of variable duration in up to 80% of NET patients with hepatic metastases. Although studies comparing RFA to other modalities are limited, RFA has been advocated in patients with bilobar disease with up to 14 hepatic lesions of less than 7 cm in diameter, encompassing up to 20% of liver volume.33,39 TAE and TACE appear to deliver comparable results and thus one modality is not favoured over the other. Embolisation is usually indicated for more extensive hepatic disease or for tumours in close proximity to biliary structures precluding RFA.39 Duration of response is routinely short as the tumour rapidly develops collaterals and thus repeat treatments are often required.41 Embolisation is contraindicated in patients with 50–75% liver involvement due to the risk of precipitating acute hepatic failure. In general, aggressive multimodal therapy with embolic, ablative and systemic strategies is recommended to debulk or downstage metastatic NETs.41 Despite complete resection, hepatic recurrence occurs in up to 84% of patients at 5 years post-surgery.39 Recurrence is suspected by the elevation of tumour markers such as 5-hydroxyindoleacetic acid (5-HIAA) and chromogranin A. Chromogranin A is more sensitive than 5-HIAA in identifying disease progression and high levels have been shown to predict poorer outcomes. A reduction in chromogranin A levels of > 80% predicts a good outcome following cytoreductive hepatectomy, even when complete resection has not been achieved.42 Liver transplantation has been advocated for patients with extensive, unresectable liver metastases with no extrahepatic disease. A recent retrospective study of 150 patients who underwent transplantation for metastatic NETs reported 5-year survival comparable to patients with hepatocellular carcinoma (HCC).43 Of those transplanted, patients under the age of 55 without the need for concurrent major resection of the primary tumour had the best overall survival.9 Therefore, liver transplantation does appear to confer long-term survival in carefully selected patients and should be considered in the management of NETs.44 Gastrointestinal stromal tumours (GISTs) are the most common gastrointestinal mesenchymal malignancies originating from the interstitial cells of Cajal. Approximately 70–80% of GISTs harbour a mutated c-Kit proto-oncogene, which results in the constitutive activation of the receptor tyrosine kinase and unregulated cell growth. Two thirds of c-Kit mutations are located on exon 11.45 C-Kit exon 9 and PDGFRA mutations, encompassing a wild-type kinase domain that modulates receptor inhibitor sensitivity, account for another 5–10% of GISTs.46 Primary GISTs represent 1% of all gastrointestinal malignancies, and arise in the stomach (55%), small intestine (35%), colon/ rectum (10%) and oesophagus (5%), with the remainder found in various other sites (gallbladder, appendix or mesentery).47 The primary tumour is usually classified into four prognostic categories, ranging from very low risk to high risk, according to site of the lesion, size of the lesion and the number of mitotic figures identified.48 Surgery remains the gold standard for the treatment of primary GISTs. Imatinib mesylate is a selective tyrosine kinase inhibitor that has revolutionised the treatment of unresectable GISTs.44 Response to imatinib is greatest in tumours that harbour the c-Kit exon 11 mutation, with resistance rates higher in patients harbouring exon 9 or platelet-derived growth factor receptor α (PDGFRA) mutations.44 Despite complete surgical resection with microscopic negative margins, recurrence (local or distant) occurs in 50% of patients.48 The use of imatinib in the adjuvant setting was investigated in the phase III ACOSOG placebo controlled trial (Z9001) for patients with resected GISTs 3 cm or greater in size. A statistically significant 1-year recurrence-free survival (RFS) of 98% in the treatment group versus 83% in the placebo group was observed, prompting the inclusion of imatinib as an adjuvant treatment modality.48 Currently, many nomograms have emerged to guide patient selection for those believed to be at highest risk of recurrence. The treatment of metastatic GISTs has similarly been transformed by imatinib. Recurrence of GISTs most commonly occur with one of two metastatic patterns: local recurrence with peritoneal disease or intraparenchymal liver metastases.49 Most patients with recurrent metastatic GISTs will receive imatinib as first-line treatment, with a clinical response demonstrated in 80%. This response is durable with a median survival of 48 months.50 However, many patients develop imatinib resistance and disease progression caused by the development of secondary mutations.51 Second- (e.g. sunitinib) and third-line agents (e.g. nilotinib and masitinib) have shown promise in patients resistant to imatinib.52 The efficacy and low side-effect profile of imatinib prompted initial enthusiasm for the combined use of surgery and imatinib in the management of metastatic GISTs. Although evidence guiding surgical management in metastatic GISTs is limited, a recent study combining neoadjuvant imitanib with surgery and adjuvant imitanib in patients with previous R0 resection of the primary tumour has shown a favourable 3-year survival.53 Nevertheless, future studies are warranted prior to recommending adjuvant imitanib in routine clinical practice for metastatic GISTs to the liver. A subset of patients with GISTs develop a pattern of disease progression where isolated nodular foci progress within a pre-existing tumour mass in a patient already on imatinib. Such cases of partial progression have the same median survival as patients who meet standard criteria for disease progression.54
Non-colorectal hepatic metastases
Introduction

Pathophysiology and molecular basis of liver metastases
Clinical approach to non-colorectal liver metastases
Treatment strategies
Neuroendocrine tumours


Gastrointestinal stromal tumours

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Abdominal Key
Fastest Abdominal Insight Engine



