This article presents a fair and balanced review of natural orifice translumenal endoscopic surgery. The article chronicles the history and technical aspects of natural orifice translumenal endoscopic surgery with particular emphasis on its application in urology. It is hoped that this article serves as a straightforward and pragmatic reference for practicing and academic urologists.
Evolution is defined as a process of “change in a certain direction” or ‘the process of working out or developing.” Conversely, revolution is defined as “a fundamental change in the way of thinking about something…a change in paradigm” Whether natural orifice translumenal endoscopic surgery (NOTES) is best defined as evolutionary or revolutionary is debatable. On its most basic level, NOTES is simply a means of accessing the peritoneal cavity and organs by inserting a flexible endoscopic device through a natural orifice followed by incision through the lumenal wall. In reality, NOTES constitutes a fundamental change in how urologists think about and approach minimally invasive surgery. This conceptual transformation remains a complicated and tedious work in progress because the surgical skill set and dedicated instrumentation required to perform NOTES safely and reproducibly have yet fully to arrive. Regardless, the enthusiasm for NOTES among patients and industry is undeniable and urologists must be prepared to address questions from patients and colleagues regarding the role of NOTES in managing urologic diseases. This article provides a brief history of NOTES, summarizes the salient literature, offers a pragmatic overview of the technical aspects of NOTES, and addresses the inevitable concerns regarding this or any new revolutionary technique.
History of natural orifice translumenal endoscopic surgery
The concept of using a natural orifice for expedient surgical access or specimen extraction is extremely familiar to urologists and gastroenterologists. Indeed, transurethral and peroral diagnostic and therapeutic procedures represent the sine qua non of urology and gastroenterology, respectively. It holds that urologists and gastroenterologists stand at the forefront of NOTES research.
Before Kalloo and coworkers’ landmark description of transgastric peritoneoscopy, Breda and colleagues reported removal of an intact tuberculous kidney through a posterior colpotomy to reduce morbidity and pain and improve cosmesis. Nearly a decade later, Gill and colleagues at the Cleveland Clinic detailed the successful transvaginal extraction of intact laparoscopic radical nephrectomy specimens in 10 patients. Although both Gill and Breda performed hybrid procedures (standard laparoscopy was performed to complete the operation after which specimen extraction was performed through a natural orifice), the model of using a natural orifice to improve patient outcomes was established and arguably justified.
In 2002, Gettman and coworkers published his experimental application of natural orifice nephrectomy in the porcine model. Using the transvaginal approach, six laparoscopic nephrectomies were performed, one of which was completed entirely through the vagina with the remaining five procedures performed with the assistance of a 5-mm laparoscope placed transabdominally (“hybrid” natural orifice surgery). Articulating laparoscopic instruments were used to ease technical constraints associated with in-line transvaginal placement. Operative time for the one pure transvaginal nephrectomy was 360 minutes. Mean operative time for the remaining hybrid procedures was 210 minutes. Mean blood loss was 30 mL excluding one catastrophic vascular injury that resulted in exsanguination and death. No additional perioperative complications were noted. The authors concluded that hybrid NOTES nephrectomy was feasible and reproducible in the porcine model but conceded that complete or pure transvaginal nephrectomy was, at that time, compromised by ill-adapted instrumentation and was not yet ready for human application.
Building on the aforementioned studies, Kalloo and colleagues successfully performed transgastric peritoneoscopy with or without liver biopsy in the porcine model in 2004. No immediate perioperative complications were noted and all survival animals thrived postoperatively. To address concerns of postgastrotomy bacterial contamination, postsacrifice peritoneal cultures were performed. Results were negative in most animals. The favorable results of this study generated considerable enthusiasm for NOTES and sparked a veritable litany of noncomparative diagnostic and therapeutic animal experiments including cholecystectomy, appendectomy, gastrojejunostomy, tubal ligation, and oophorectomy.
Following this abundance of successful animal experiments, a consortium of gastroenterologists and general surgeons was convened to address frankly the benefits and limitations of NOTES. A white paper was generated during this meeting and the consortium was labeled the Natural Orifice Surgery Consortium for Assessment and Research (NOSCAR). The consensus of this collaborative effort was that thoughtful and dedicated innovation is required to drive the field of NOTES forward, that NOTES research must be closely overseen by both local Institutional Review Boards and NOSCAR, and that technical limitations represented the most significant barrier to its safe application in humans. In response to, and in accordance with, the recommendations of NOSCAR, additional animal experiments were performed transgastrically, transvaginally, and transvesically, and instrumentation and operating platforms were refined.
The first human experience with NOTES was reported by Rao and Reddy in India during which transgastric appendectomy, tubal ligation, and cholecystectomy were performed. Although greater than 20 human NOTES procedures have been performed, this series has not yet been published. Although it remains difficult to accurately catalog all human NOTES procedures performed because of poor or ambiguous reporting, one can reliably state that transgastric, transvaginal, and transvesical peritoneoscopy, transgastric cholecystectomy, appendectomy, liver biopsy, and tubal ligation, and transvaginal appendectomy have all been successfully performed.
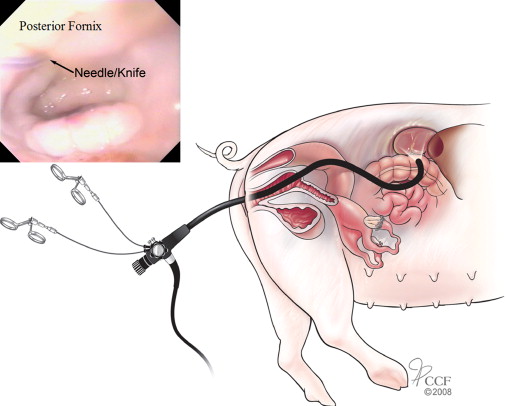
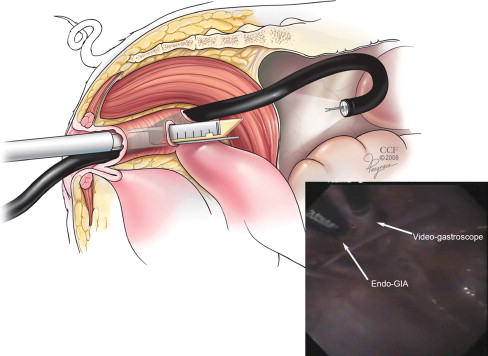
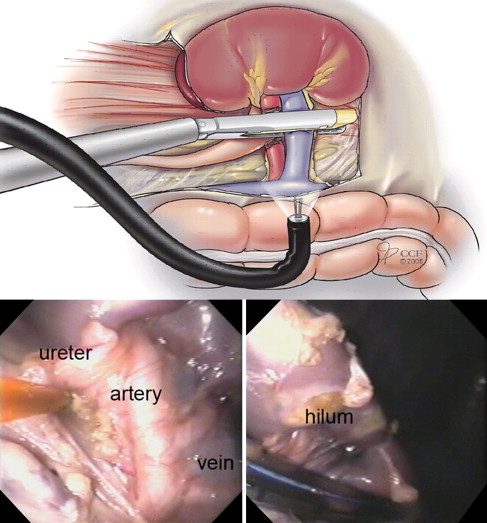
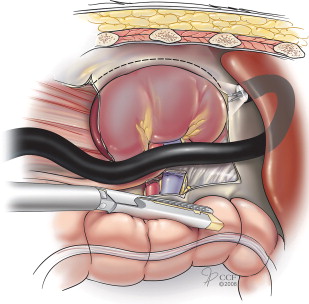
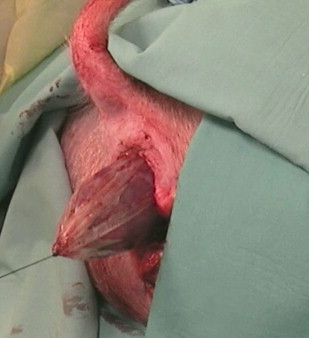
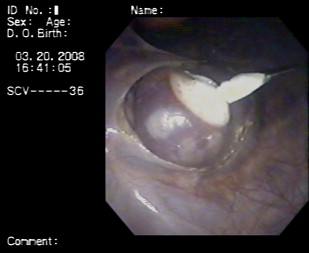
Germane to urology, experience with NOTES has been relatively limited with the plurality of experiments confined to kidney surgery in the porcine model. Multiple centers have reported successful NOTES nephrectomy. In addition to Gettman’s aforementioned experience with transvaginal NOTES nephrectomy, Mathes and colleagues reported transgastric and transvaginal nephrectomy in 2007. Using a dual-channel gastroscope, the left kidney was dissected and the renal hilum controlled with metallic clips. The kidney was morcellated and extracted. The animals were followed postoperatively with no clinical signs of abdominal infection at 19 days. Representative schematics and images of NOTES nephrectomy are found in Figs. 1–5 .
Clayman and coworkers at the University of California-Irvine presented and later published their experience with transvaginal NOTES nephrectomy in 2007. Using a specially designed operating platform, an acute experiment was performed in a female farm pig in which a 12-mm trocar was placed transabdominally through the midline with the operating platform placed transvaginally. Following dissection of the kidney through the transvaginal port, the renal hilum was controlled with an endovascular stapler deployed through the transabdominal trocar. The kidney was placed in an endoscopic retrieval bag and brought out through the vagina. This report received considerable commendation at the annual meeting of the American Urological Association and generated significant enthusiasm about the role of NOTES in urology.
In 2008, Crouzet and colleagues reported bilateral transgastric and transvesical renal cryoablation in two female farm pigs ( Fig. 6 ). The authors suggested that not only does NOTES and the use of flexible endoscopic instruments afford access to portions of the kidney that would otherwise be difficult to approach, but that cryoablation may also represent a natural transition into NOTES surgery because limited dissection and reconstruction are needed. Indeed, the ability to perform difficult dissection or reconstruction during NOTES is viewed as a major impediment to its practical application.
In response to the poor instrumentation available to perform stapling, dissecting, and suturing during NOTES, Box and colleagues reported their experience with combined transcolonic and transvaginal, single-port, robot-assisted NOTES nephrectomy. An acute experiment was performed in a female farm pig in which a 12-mm trocar was placed transabdominally in the midline and two additional 12-mm ports were placed into the peritoneal cavity through the vagina and colon. The robot was docked with a port-in-port configuration. The robotic camera was placed in the midline with grasping and dissecting instruments placed through the colon and vagina. The nephrectomy was successfully performed with minimal blood loss and without complications.
Haber and colleagues also applied the existing robotic platform during NOTES extirpative and reconstructive surgery in a porcine model. The authors successfully completed bilateral partial nephrectomy, bilateral dismembered pyeloplasty, and completion bilateral radical nephrectomy on 10 female farm pigs. In this hybrid set-up, the robotic camera and first arm were placed through the umbilicus, whereas the second arm was introduced through a posterior colpotomy ( Figs. 7 and 8 ). Mean operative time was 154 minutes (range, 140–187 minutes). Mean estimated blood loss was 73 mL (range, 55–100 mL). No intraoperative complications were encountered and no technical constraints or robotic system failures occurred during either right- or left-sided procedures. The authors concluded that use of the robotic platform may overcome the learning curve and technical obstacles associated with NOTES.


In 2007, Gettman and Blute successfully performed transvesical peritoneoscopy on a 56-year-old man before robotic prostatectomy. Under confirmatory standard laparoscopic guidance, an injection needle was used to perforate the bladder wall through which a flexible ureteroscope was passed. The peritoneal cavity was surveyed adequately and completely. The cystotomy was closed robotically before prostatectomy. No intraoperative or postoperative complications were reported.
In 2009, Kaouk and colleagues at the Cleveland Clinic successfully performed the world’s first transvaginal NOTES nephrectomy on a 57 year old female with a non-functioning right kidney. Following insufflation with a Veress needle, a camera was introduced into the abdominal cavity through a 5 mm umbilical port to allow vaginal access under direct vision. Using a standard GelPort ® positioned through a 3 cm colpotomy, the kidney was dissected, the renal hilum exposed and controlled, and the kidney extracted exclusively through the vaginal incision. Operative time was 307 minutes. Estimated blood loss was 100 mL. No intraoperative complications occurred.
Natural Orifice Translumenal Endoscopic Surgery Access
NOTES has thus far been successfully completed experimentally by the transgastric, transvaginal, transcolonic, and transvesical routes. Although strikingly singular organs, the logistics of transvisceral surgery are universal. First, a natural orifice (mouth, anus, vagina, or urethra) is accessed with aid of a flexible multichannel videoscope (gastroscope, ureteroscope, or laparoscope). An incision is made through the stomach, colon, vagina, or bladder using a needle knife and a wire is passed into the peritoneal cavity using a modified Seldinger technique ( Fig. 9 ). A radially dilating balloon is variably used to enlarge the access tract ( Fig. 10 ). A catheter, guide tube, or overtube is placed over the guidewire and insufflation is achieved with CO 2 . A multichannel videoscope is then advanced further into the peritoneal cavity and the diagnostic or therapeutic procedure performed with flexible operating instruments ( Fig. 11 ). The viscerotomy is closed at the termination of the procedure. Although seemingly straight-forward, this step-wise approach to NOTES is overly simplistic and a dedicated evaluation of each access route and its comparative merits deserves mention.








