Port Placement
■ Initial trochar placement: open Hasson approach at a periumbilical position, Veress needle approach in left upper quadrant, or optical separator approach in the left upper quadrant
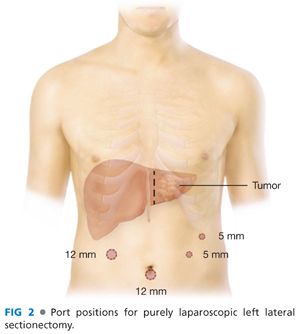
■ FIG 2 shows the suggested port positions for a purely laparoscopic left lateral sectionectomy. A 12-mm port at the periumbilical incision, a 12-mm port in left upper quadrant midclavicular line for laparoscopic ultrasound and Endo GIA stapler, a 5-mm port in left upper quadrant midclavicular line, and a 5-mm left subcostal/left flank port.
Mobilization of the Left Lateral Segment
■ Using a thermal energy device of choice through the right upper quadrant 12-mm port, divide the round ligament at the abdominal wall. The assistant provides countertension through the left-sided 5-mm ports.
■ Using hook cautery through the right upper quadrant 12-mm port, divide the falciform ligament toward the insertion of hepatic veins into the inferior vena cava (IVC). The assistant provides countertension through the left-sided 5-mm ports by compressing the liver posteriorly and inferiorly. The avascular adventitia protecting the hepatic veins should be divided to fully expose the anterior aspect of the common trunk of the middle and left hepatic vein.
■ Using the hook cautery through the left upper quadrant 5-mm port, divide the left triangular ligament. Optional: Protect the stomach and spleen with a 4 × 4 gauze between the left triangular ligament and stomach.
■ Using the hook cautery through the left-sided ports, divide the hepatogastric ligament, and identify any replaced or accessory left hepatic artery. The assistant lifts the left lateral section through the right upper quadrant 12-mm port. Clip and ligate any replaced/accessory left hepatic artery.
■ Rarely, obtaining an adequate margin will dictate extraparenchymal dissection of the portal structures supplying segments 2 and 3. The author’s favored approach is to identify the left hepatic artery near the porta hepatis and dissect it distally to identify and divide the segmental branches of all of the portal structures.
Parenchymal Transection of the Liver
■ Ultrasound the liver and ensure that the liver mass(es) is/are localized only in the left lateral sector of the liver and that the transection plane achieves an adequate oncologic margin (≥1 cm).
■ Mark the transection plane just to the left of falciform ligament with the hook cautery.
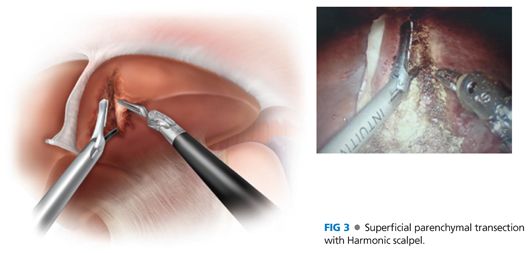
■ The first 2 cm of parenchymal depth can be divided safely with an energy device of choice (FIG 3). The optimal trajectory for the liver parenchymal transection is through the right upper quadrant 12-mm port heading toward the insertion of the left hepatic vein. The camera is at the periumbilical port and the assistant uses an atraumatic grasper and suction/irrigator from the left-sided 5-mm ports.
■ As the dissection progresses deeper into the parenchyma, expect to encounter the crossing segments 2 and 3 portal veins, biliary branches, and hepatic vein branches. Using a flat, blunt instrument (e.g., laparoscopic bowel grasper), create a tunnel in the liver parenchyma below these crossing branches (FIG 4). The tunnels creates an easy path for the Endo GIA stapler (2.5-mm vascular loads are preferred) (FIG 5). The blunt instrument and lower blade of the stapler should easily slide through liver parenchyma. If the instrument meets resistance, it suggests a crossing vascular or biliary branch along that path and the instrument needs to be redirected. The last division to free the liver section is the division of the left hepatic vein approximately 2 cm from the insertion into the IVC with Endo GIA vascular load.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


