Fig. 9.1
The Crawford set
9.2.1.1 Stenting Placement
Each punctum should be dilated. The lacrimal system is probed to open any blockages by using a standard lacrimal probe such as a Bowman 00.
The Crawford probe is passed through the upper punctum and across the upper canaliculus and then oriented down through the lacrimal system into the nose approximately 4 cm.
The probe is located in the nose using the Crawford Retrieval Hook. Note that the flat on the hook handle indicates the orientation of the hook in the nose.
The wire is touched by the hook and then engaged by rotating the hook 90° in the direction of the wire. The probe is pulled back to nest the olive tip of the probe in the hook. Using the hook, the probe is pulled from the nose (Fig. 9.2).

Fig. 9.2
Crawford stenting placement
Often a push/pull technique and some working of the hook with the wire will be required to complete the intubation.
The second probe is passed down the inferior canaliculus and out of the nose in a similar fashion.
When the silicon tube is correctly placed, the wire probes are removed and the silicone tubes placed under slight tension using a clamp with tubing that protected the jaws, and the tubing itself is tied and the knotted silicone tubing secured by a fine suture of the surgeon’s choice, for example, 8–0 silk. The knotted tubes are then tucked up into the nose. Because of the bulk of the knot, it will not pass through the canaliculus, and the tubes must be removed through the nose [1, 3, 4].
9.2.2 Nunchaku-Style Tube
The Nunchaku-style silicone tube is an example of bicanalicular nasolacrimal intubation that is indicated for canalicular pathologies, congenital nasolacrimal duct obstruction, and dacryocystorhinostomy (DCR).
Intubations with other silicone tubes, such as Crawford’s tube, are commonly used, but these tubes need to be retrieved from the patient’s nose. Instead with the Nunchaku-style tube, retrieval from the nose is unnecessary, because it is more flexible and stable than other silicone tubes. In addition, it is a less invasive treatment for lacrimal passage obstructions, and the physiologic anatomy of the lacrimal passage remains intact.
It is 105 mm in length and has a central thin segment (25 mm in length and 0.6 mm in diameter) and a bilateral thick segment (40 mm in length, 0.5 mm inner diameter, and 1.0 mm outer diameter); it looks like the “Nunchaku” used by Chinese martial arts practitioners. The bilateral tubes are slit 30 mm from the closed points of the bilateral tube segments. A stainless steel probe (55 mm in length) with a polypropylene grip is inserted through each slit. So the metallic guides are located inside the lumen, not as an extension of the stent as in conventional intubation sets (Fig. 9.3).
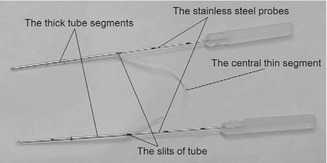
Fig. 9.3
Nunchaku-style tube
9.2.2.1 Stenting Placement
This kind of intubation can be performed as a blind procedure or under dacryoendoscopic control, in order to relieve obstructions under direct visualization and easily to avoid false intubations.
After anesthetizing the upper and lower puncta and performing an infratrochlear nerve block with 2 % lidocaine, both puncta are enlarged using a punctal dilator. The probe of the dacryoendoscope is inserted through the upper canaliculus. Upon reaching the lacrimal sac, the probe is thrust forward into the nasolacrimal duct to relieve the obstructions under direct visualization.
During this procedure, saline can be injected through the water channel to remove hemorrhage and to create space.
After relieving the obstruction by the dacryoendoscopy probe, one end of the Nunchaku-style tube is inserted into the upper puncta. When it reaches the medial wall of the nasolacrimal sac through the canaliculus, it is turned vertically and then inserted into the nasolacrimal duct and nasal cavity. The stainless steel probe inside the tube is then pulled out. After insertion of the tube into the upper puncta, the other side of the Nunchaku-style tube is inserted through the lower puncta in the same way.
Finally, it is possible to confirm that the silicone tube has been correctly intubated using the dacryoendoscope from the upper or lower puncta [2].
9.2.3 The Ritleng Method
There are several intubation sets for bicanalicular silicone intubation. In one type of set, silicone tubing is bonded to a metal probe ranging in length from 114 to 177 mm. Difficulty of retrieval of the metal probes from the nose and associated mucosal injury is the main disadvantage of these sets. Instead in the Ritleng intubation technique, the silicone tube is attached to a Prolene suture that serves as a guide, and it seems to be easier and less traumatic to retrieve a Prolene suture from the inferior meatus than a metal probe [5].
The Ritleng probe is a straight tube, rigid and hollow, measuring 1 mm in diameter and 105 mm long. It has a 0.3 mm-wide slit running its full length and an opening at each end.
A slight curve to the distal part of the probe can be given, thus conforming it to the angle between the superomedial orbit and nasolacrimal duct (Fig. 9.4).
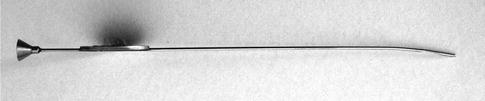
Fig. 9.4
The Ritleng probe
In the Ritleng intubation set, each end of the silicone tubing is threaded onto a Prolene monofilament suture material. This is composed of a thicker dark blue initial portion bonded to the silicone tubing, a thinner light blue middle portion, and a thicker dark blue free end (Fig. 9.5).
Fig. 9.5
The Ritleng intubation set
Only the thinner middle portion of the Prolene can slip out of the slit of the probe.
All intubations are performed by or under supervision of one surgeon, under general endotracheal anesthesia.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


