Hepatic Segmental Resections
William R. Jarnagin
Charbel Sandroussi
Paul D. Greig
Introduction
Better understanding of hepatic anatomy has been pivotal in the evolution of safe liver surgery (see Chapter 18 and Figs. 17.6, 18.6 and 23.1). Compared to lobar and extended lobar resections, segmental liver resections, where appropriate, allow preservation of liver parenchyma without compromising oncologic results. The ability to resect one or two segments rather than the entire lobe allows parenchymal preservation, which is critical in patients with diseased parenchyma and in those with extensive disease and/ or a high likelihood of requiring future liver directed therapy. The latter are particularly relevant in patients with metastatic disease. Segmental vascular inflow control may facilitate the resection by precisely mapping the transection plane, although this is not always possible. In addition, such anatomically based resections involving the removal of a hepatic segment confined by tumor-bearing portal tributaries may, in fact, be more sound from an oncologic standpoint.
Anatomy and Terminology
The segmental anatomy of the liver originated from the original descriptions of Couinaud in 1952. Couinaud’s work showed that the liver consists of eight independent segments, each with its own vascular inflow, hepatic venous outflow, and biliary drainage and each amenable to resection. These segments form the foundation of current hepatic nomenclature (Fig. 24.1A and B; see also Fig. 18.6). The Brisbane Terminology eliminates confusing terminology of lobes and sectors used in past descriptions of liver anatomy. The terms hemi-liver (first order division), section (second order division), and segments (third order division) are not interchangeable and provides common terminology for better communication among surgeons, radiologists, and other physicians.
The first order division separates the right (segments 5 to 8) and left (segments 1 to 4) hemi-livers (or liver) along the principal resection plane or Cantlie’s line, delineated by the middle hepatic vein (MHV), coursing along a line from the gallbladder fossa to the IVC. The second order division separates the right and left hemi-livers into liver
sections based on the portal distribution (i.e., the primary divisions of the right and left portal pedicles) and the hepatic venous drainage. The right liver is divided into right anterior (segments 5 and 8), and right posterior (segments 6 and 7) sections, separated by the right hepatic vein (RHV). The left liver is divided into left lateral (segments 2 and 3) and left medial (segments 4a and 4b) sections by the umbilical vein, which runs along a line delineated by the falciform ligament. Together, segments 2 and 3 are commonly, but erroneously, referred to as the left lateral segment.
sections based on the portal distribution (i.e., the primary divisions of the right and left portal pedicles) and the hepatic venous drainage. The right liver is divided into right anterior (segments 5 and 8), and right posterior (segments 6 and 7) sections, separated by the right hepatic vein (RHV). The left liver is divided into left lateral (segments 2 and 3) and left medial (segments 4a and 4b) sections by the umbilical vein, which runs along a line delineated by the falciform ligament. Together, segments 2 and 3 are commonly, but erroneously, referred to as the left lateral segment.
 Figure 24.1 A: Axial CT scan image through the upper liver demonstrating the anatomic boundaries of segments 1, 2, 4a, 8, and 7. B: Axial CT scan image through the lower liver demonstrating the anatomic boundaries of segments 1, 3, 4b, 5, and 6. RHV, right hepatic vein; MHV, middle hepatic vein; LHV, left hepatic vein. From: W.R. Jarnagin (ed.), Blumgart’s Surgery of the Liver, Biliary Tract and Pancreas, 5th Edition, Elsevier, 2012. |
The third order division separates segments into segments (numbers 1 to 8) and is defined by hepatic arterial supply and biliary drainage (see Figs. 17.6 and 18.6).
Selection of Patients
Anatomically based resections should be the gold standard in most cases, excluding fenestration of liver cysts (see Chapter 28), wedge excisions of superficial lesions, and enucleation of certain lesions such as metastatic neuroendocrine tumors (see Chapter 25). A clear understanding of the patient’s segmental liver anatomy is essential to a safe, controlled resection. Segmental resections are not limited by indication nor by the presence of hepatic parenchymal disease.
Achieving a balance between parenchymal sparing resections and adequate tumor clearance is clearly an important consideration for all resections but is critical in patients with diseased livers. In patients with hepatocellular carcinoma (HCC), where cirrhosis is frequently present, segmental liver resection forms a bridge between the major hepatectomy and non-anatomic resection to preserve the maximum liver volume to prevent postoperative liver failure. Since HCC have a propensity for intraportal extension and dissemination, segmental resections, by removing the parenchyma supplied by the principal segmental portal vein branch, are likely to be more effective than non-anatomic resections from an oncologic standpoint. Segmental liver resection is also preferred in patients with multifocal colorectal metastasis treated extensively with preoperative chemotherapy, which frequently results in hepatic dysfunction and impaired regeneration due to steatosis (see Fig. 18.1).
 PREOPERATIVE PLANNING
PREOPERATIVE PLANNINGThe planning of a segmental-based resection must take into account anatomic variations and their relationship to the plane of transection (Fig. 24.2) (see Figs. 17.9, 19.2, and 21.1, 21.2, 21.3 and 21.4). Resection has been facilitated by the precision digital imaging provided by computerized tomography, magnetic resonance imaging (MRI), and ultrasound (US), allowing interpretation of intrahepatic vascular and biliary anatomy (see Chapter 18) and the ability to manipulate and scroll through reconstructions in the axial, coronal, or sagittal planes using software such as picture archiving and communication system
(PACS). With the appropriate protocol for arterial and venous enhancement, the third and fourth level vascular structures can be accurately defined. More sophisticated software is available that may facilitate the preoperative planning. These easily manipulated, three-dimensional reconstructions that create a virtual reproduction of the liver can be used to determine the proposed plane of transection, taking into account the minimum resection margin, and residual volume of liver (Fig. 24.3).
(PACS). With the appropriate protocol for arterial and venous enhancement, the third and fourth level vascular structures can be accurately defined. More sophisticated software is available that may facilitate the preoperative planning. These easily manipulated, three-dimensional reconstructions that create a virtual reproduction of the liver can be used to determine the proposed plane of transection, taking into account the minimum resection margin, and residual volume of liver (Fig. 24.3).
 Figure 24.2 Axial CT image showing variant portal venous anatomy, with the left portal vein (LPV) arising as a branch of the right anterior sectoral branch (Ant PV) and the posterior sectoral branch (Post PV) branching separately from the main portal vein (MPV). |
General Operative Principles
Preoperative Assessment and Anesthesia
The preoperative assessment and preparation of the patient for a liver resection are described in Chapter 18. Comorbidities should be identified and optimized. Careful assessment of liver function, particularly in those with intrinsic liver disease is important. Preoperative biliary decompression and/or portal vein embolization are infrequently required for patients undergoing segmental compared to more extensive resections (see Chapters 18, 19, 20, and 26). Particular attention should be paid to the reduction of the central venous pressure during transection in order to reduce blood loss, and measures to prevent hypothermia, infections, and venous thromboembolism are required.
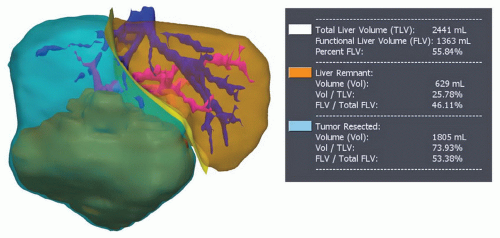 Figure 24.3 Three-dimensional model generated from a preoperative CT scan using ScoutTM software system (Pathfinder Therapeutics, Inc, Nashville, TN). The planned resection plane is shown. The total liver volume, the functional liver volume (total volume—tumor volume), and future liver remnant volumes are shown. |
Exposure and Mobilization
Segmental resections may be performed laparoscopically (see Chapter 31) or at laparotomy. For open resections, exposure can be achieved through a variety of incisions (see Figs. 18.7, 19.3 and 21.5), including right subcostal with midline extension (hockey-stick) or its modification (J-shaped), or a bilateral subcostal incision with (Mercedes incision) or without (chevron) midline extension. A long midline incision may be used for selected liver resections, particularly if combined with a left or sigmoid colon or rectal resection; thoracoabdominal is seldom required. Following laparotomy and general inspection, the liver is mobilized by transection of the obliterated umbilical vein and division of the falciform ligament as it triangulates onto the IVC to identify the origins of the hepatic veins (see Fig. 19.4). Mobilization of the right and left livers requires division of the triangular ligaments in order to free the liver fully from the hemidiaphragms. During the division of the lesser omentum (gastro-hepatic ligament), attention should be given to the presence of an accessory or replaced left hepatic artery arising from the left gastric artery (see Chapter 20). Full mobilization of the right liver requires division of the coronary ligaments; if resection of one of the posterior right segments is planned (6 and/or 7), then the right adrenal gland must be separated and allowed to retract into the retroperitoneum and dissection of the retrohepatic IVC must be performed, as one would for more extensive procedures (see Chapters 19 and 23, Figs. 19.5, 19.6, and 23.12).
Intraoperative Assessment
The intraoperative assessment of the liver requires correlation of the findings of inspection and palpation of the mobilized liver with those of the preoperative imaging (see Chapter 18). Intraoperative ultrasound is used to localize the lesion, confirm the preoperative imaging findings, and further stage the proposed remnant liver (see Fig. 18.9




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
