Chapter 90B Hepatic resection for benign disease and for liver and biliary tumors
Overview
Hepatic resection for removal of lesions of the liver may be necessary for a wide variety of conditions (Box 90B.1). Indications for partial hepatectomy include the treatment of primary benign or malignant growths of the liver and biliary tract or metastatic tumors, with the latter being the most common. Hepatic resection also may be necessary in the management of complex or symptomatic cystic disease involving the liver (see Chapter 68, Chapter 69A, Chapter 69B ) and to allow access for repair of selected benign biliary strictures (see Chapter 42A, Chapter 42B ). Liver resection occasionally is necessary in the management of hepatic trauma. More recently, liver resection in living donors has been used in liver transplantation (see Chapter 98B).
Box 90B.1 Most Common Conditions for Which Liver Resection May Be Used
The principles of segmental and subsegmental resection are not new (Nagasue et al, 1985), and they have been developed and refined through the years. Utilization of intraoperative ultrasound (IOUS) (Bismuth & Castaing, 1984; Castaing et al, 1985; Scheele, 1989) to identify intrahepatic structures (see Chapter 21) and a mastery of intrahepatic anatomy are paramount to performing safe resections. This chapter focuses on major resections, including right hepatectomy, left hepatectomy, and extended right (including segment IV) and left hepatectomy (including the right anterior sector). Commonly performed segmental resections, including caudate lobe resection, are briefly described. A more detailed description of segment-oriented resection of the liver is provided in Chapter 92.
Hepatic resection in patients with cirrhosis is further complicated by the presence of portal hypertension and a concomitant functional deficit of the future liver remnant (FLR) (see Chapter 90F). Liver resection for the removal of gallbladder carcinoma and cholangiocarcinoma at the confluence of the bile ducts can be especially troublesome in the postoperative period, because resection is frequently performed in the presence of biliary obstruction, bacterial contamination, and infection.
General Principles
Benign Disease
Partial hepatectomy for the removal of benign tumors or cysts of the liver generally should be performed only for symptomatic patients, in the presence of doubt as to the diagnosis, or for tumors with known malignant potential (see Chapter 79A, Chapter 79B ). Removal of normal liver tissue should be kept to a minimum, thus when intervening for benign lesions, use of techniques for enucleation should be considered. Such enucleative methods may be utilized in the management of hemangioma, adenoma, and fibronodular hyperplasia. Enucleation also may be appropriate for tumor debulking of metastatic neuroendocrine tumors. The technique and principles of enucleation are described in the operation of pericystectomy for the removal of hydatid cysts of the liver (see Chapter 68).
Liver resection may be necessary in the management of some complex benign biliary strictures, especially when associated with ipsilateral liver atrophy (see Chapter 42A, Chapter 42B ). Some benign biliary conditions that sometimes necessitate resection include intrahepatic stones associated with recurrent pyogenic cholangitis (see Chapter 44) and Caroli disease, a congenital cystic disease of the liver (see Chapter 46, Chapter 69A, Chapter 69B ). In these situations, the amount of normal hepatic parenchyma removed should be kept to a minimum in accomplishing the goal of the resection. Liver resection for hydatid disease is discussed in Chapter 68, and resection for hepatic trauma is discussed in Chapter 102.
Malignant Disease
When performing partial hepatectomy for malignant tumors, the guiding principle is to obtain negative margins of resection while maintaining patient safety. Ideally, the closest margin distance from the tumor edge should be approximately 1 cm (Are et al, 2007); however, the margin distance must often be sacrificed, both for patient safety and for preservation of major vascular structures in close proximity to the tumor that are required to sustain the future liver remnant. That said, complete resection with a close margin is still associated with improved survival, and thus the inability to obtain a wide margin based on preoperative imaging should not necessarily be a deterrent to resection (Pawlik et al, 2005; Poultsides et al, 2010). Furthermore, an effort should always be made to perform parenchyma-sparing resections without sacrificing oncologic efficacy.
The difficulty of achieving an adequate margin of clearance when performing wedge resections for peripherally situated tumors should not be underestimated. The deep margin is the most difficult to judge for adequate tumor clearance. Consequently, it has been shown that wedge resections can carry an unacceptable local recurrence rate (DeMatteo et al, 2000; Gall & Scheele, 1986), although this has not been universally observed (Zorzi et al, 2006). Another factor that may compromise wedge resections is the fact that the liver has a tendency to fracture at the interface between tumor and normal parenchyma. This is particularly a problem for hard tumors in a soft liver, as is often the case with metastatic colorectal carcinoma; thus the surgeon must maintain extreme caution during parenchymal transection for wedge resections to avoid a close margin, a problem best averted by transecting along anatomic planes defined by inflow and outflow structures.
Patients undergoing palliative resections for metastatic neuroendocrine tumors that are not amenable to complete resection may be good candidates for enucleation, as is often done for benign lesions (see Chapter 81B). Gallbladder carcinoma and cholangiocarcinoma situated at the confluence of the hepatic bile ducts frequently occlude biliary flow, and resection may be compromised not only by the adverse pathophysiology of obstructive jaundice, but also by infection that may have been introduced before operation as a result of either percutaneous or endoscopic stent placement. In addition, perioperative outcome is complicated by the concomitant partial hepatectomy and resection of the extrahepatic biliary apparatus and subsequent biliary reconstruction (see Chapter 50B).
The presence of cirrhosis also introduces unique challenges for performing liver resection. Preoperatively, appropriate patient selection is paramount to ensure that the FLR is adequate and that the patient will be able to tolerate the procedure. Intraoperatively, a firm, nodular, and enlarged liver poses technical difficulties in mobilization and parenchymal transection that may also contribute to increased blood loss secondary to portal hypertension. Postoperatively, the increased risk of liver insufficiency, hepatic failure, and increased susceptibility to infection are major concerns. Thus, resection should be reserved for patients with cirrhosis who have relatively preserved liver function, and the principles of parenchyma-sparing resection should be strictly followed (see Chapter 90F).
Principal Hazards
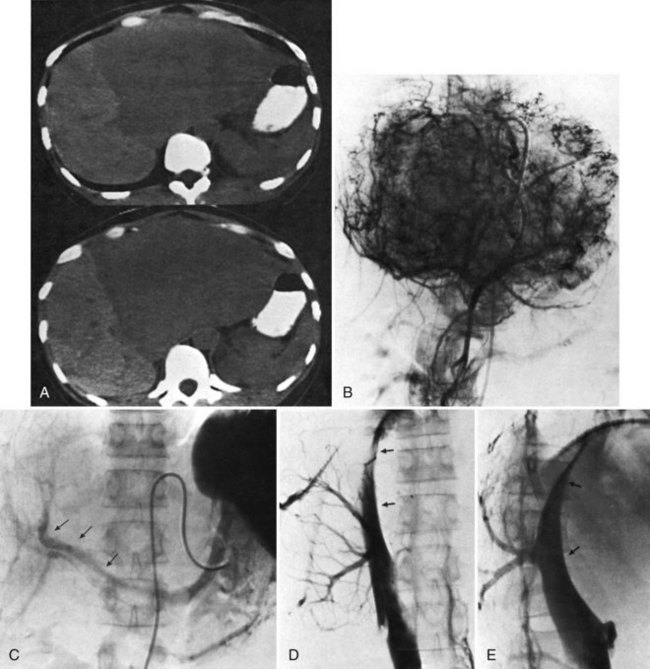
The main hazards of hepatic resection are biliary leakage and bleeding (see Chapter 25). Biliary leakage is a particular problem in patients in whom biliary reconstruction is necessary, for example, as in the removal of a hilar cholangiocarcinoma. Bleeding from the hepatic veins and the inferior vena cava (IVC) during parenchymal transection is a major concern. Bleeding is more likely to occur during major resection of superiorly and posteriorly placed tumors, where clearance is minimal between the tumor margin and the passage of the hepatic veins into the vena cava, or when tumors are closely adherent or adjacent to the IVC (Fig. 90B.1).
Future Liver Remnant
A healthy, noncirrhotic liver may tolerate a resection of up to 80% of its volume because the liver’s enormous regenerative capacity enables functional compensation within a few weeks (see Chapter 5; Blumgart et al, 1971); however, such a favorable response cannot be taken for granted for extended hepatic resections. Only if reduction of the functional liver parenchyma is less than 50% can the risk of clinically significant liver insufficiency be virtually disregarded. Postoperative hepatic reserve is of particular concern after an extended left hepatectomy and when all of the parenchyma to the right of the falciform ligament is removed (extended right hepatectomy, which will be discussed later). Minimal to no risk of postoperative liver failure is present if most of the specimen volume has been replaced by an extensive tumor mass. In such patients, compensatory hypertrophy of the unaffected residual liver already has occurred preoperatively, and the loss of functional parenchyma is limited; however, a comparable volume of resection performed for multiple or unfavorably located smaller lesions carries a much greater risk of postoperative liver failure. Small tumors located adjacent to the inflow or outflow vessels of multiple segments may mandate removal of large amounts of functioning parenchyma.
Recently, some have advocated the liberal use of portal vein embolization (PVE) in this situation (see Chapter 93A, Chapter 93B ; Abdalla et al, 2002; Makuuchi et al, 1990; Palavecino et al, 2009); however, evidence is insufficient to suggest that PVE is associated with improved postoperative results in patients with normal parenchyma (Farges et al, 2003). In a series of 1800 liver resections performed at Memorial Sloan-Kettering Cancer Center (MSKCC), significant postoperative liver dysfunction and associated death occurred in only six patients (Jarnagin et al, 2002). In this series, PVE was utilized sparingly, and preoperative measures of liver function were not used routinely, such as the indocyanine green retention test; however, in patients with a damaged or steatotic liver—more common in obese patients, those with diabetes, and patients who have received substantial chemotherapy—the risk of postoperative liver insufficiency and failure is increased (Behrns et al, 1998; Kooby et al, 2003a). PVE may prove to be justified in this group of patients undergoing major resections. Biliary obstruction with jaundice is common in patients with hilar cholangiocarcinoma, who also are at increased risk. PVE in these patients also may be justified in select cases (see Chapter 50B, Chapter 93A, Chapter 93B ; Seyama et al, 2003).
In the cirrhotic liver, liver regeneration is much less effective; impairment of liver function after resection is greater, may last longer, and may result in terminal liver failure. Liver failure is the most common cause of postoperative death after liver resection in patients with cirrhosis. Postoperative liver failure and postoperative mortality are related to the degree of preoperative liver decompensation and to the extent of nontumorous liver parenchyma removed. Liver failure may be precipitated by intraoperative bleeding, and a significant relationship has been found to exist between intraoperative blood loss, postoperative increase in serum bilirubin, and postoperative mortality. The occurrence of other postoperative surgical complications, such as abdominal infection, may also trigger postoperative liver failure. In addition, cirrhosis predisposes to multiorgan failure after hepatectomy. Although evidence supports the safety of major hepatic resection in cirrhotic patients with Child-Turcotte-Pugh (CTP) class A liver function (Fong et al, 1999a; Franco et al, 1990), it also suggests that PVE may improve perioperative outcomes by optimizing the FLR (Palavecino et al, 2009).
Portal Hypertension and Ascites
The formation of ascites is one of the most frequent complications seen after liver resection in cirrhotic patients, occurring in 80% of patients. The etiology is likely twofold, the result of an increase in portal hypertension and of the ligation and division of lymphatics in the hepatic pedicle and liver ligaments. Postoperative ascites is a serious complication. Gross abdominal distension can interfere with ventilatory function and may result in leakage and disruption of the abdominal incision. Leakage of large-volume ascites may also lead to major fluid, protein, and electrolyte losses. In addition, ascitic fluid may become infected, and this may be an irreversible complication that leads to patient demise. Incidentally, ascites formation can also occur after liver resection and after fenestration in patients with polycystic liver disease (see Chapter 69B).
Infection
Despite the nearly universal formation of fluid collections after liver resections, particularly in the resection bed, infection of this fluid is relatively infrequent in most patients; however, a serious risk of infection follows liver resection in patients with biliary obstruction, especially in the presence of preoperative radiologic or endoscopic manipulation, and in cirrhotic patients. Alterations of humoral and cellular immunity are thought to predispose to infection after abdominal surgery in patients with cirrhosis. This risk is particularly high in patients with ascites or jaundice (Rimola et al, 1986). We also have empirically observed a slightly increased rate of infected fluid collections in patients undergoing simultaneous resections of a colorectal primary along with the liver metastases. In these combined resections, we now often leave an intraabdominal drain near the liver resection bed.
Selection of Patients for Liver Resection
When selecting patients for liver resection, the oncologic appropriateness of the resection must be considered first and foremost, followed closely thereafter by the general condition of the patient. Once resection is determined to be reasonable, and the patient appears to be a candidate from a general health perspective, the technical aspects of the resection must then be considered, including the extent of resection and the quantity and quality of the FLR. If the tumor can be completely resected without compromising hepatic arterial and portal venous inflow, biliary drainage, and venous outflow of the remnant, and if the FLR is of sufficient size in a well-functioning liver, nearly all patients are candidates for hepatic resection. Careful consideration must be taken when deciding to perform a major resection to remove multiple or centrally situated small lesions in patients in whom compensatory hypertrophy of the residual liver has not yet occurred. The selection of patients with a benign biliary stricture for hepatic resection is described in Chapter 42A, and the role of liver resection in specific situations, such as for hilar cholangiocarcinoma and hemangioma, are described below.
When considering patients with compromised liver function or cirrhosis for hepatic resection, it is important to understand that, in addition to the disease extent and the general condition of the patient, the degree of hepatic dysfunction is a major prognostic factor. The CTP classification system (Child & Turcotte, 1964; Pugh et al, 1973) is a simple means of assessing liver function preoperatively. Although more sophisticated tests can be used (see Chapter 2), the CTP classification is sufficient for most situations. Also, a low preoperative platelet count is a good surrogate marker for portal hypertension and underlying liver disease that otherwise may not be detectable (Bruix et al, 1996; Maithel et al, 2010). Operative mortality is much higher in CTP class B or C patients compared with those with class A liver function. Liver resection is particularly hazardous in a patient with a Pugh score greater than 8 (CTP class B). Serum bilirubin concentration is also an important prognostic factor, as liver resection is ill advised in patients with a serum bilirubin greater than 2 mg/dL or in the presence of clinically detectable ascites.
The extent of hepatectomy is guided by tumor size and location, but in general, the ideal is to remove as little parenchyma as possible. Small tumors located deep in the right liver are challenging, as it is preferable to avoid performing a right hepatectomy in such cases. If right hepatectomy is necessary, preoperative PVE of the affected lobe may allow hypertrophy of the contralateral side (see Chapter 93A, Chapter 93B ); however, the utilization of alternative methods for liver-directed therapy to obtain tumor control in a cirrhotic patient should be considered, especially in patients with multifocal disease. Alcohol injection, transarterial chemoembolization—bland, conventional, and using drug-eluting beads—cryoablation, radiofrequency ablation, microwave ablation, yttrium-90 therapy, and liver transplantation for managing tumors of the liver are discussed in detail in Chapter 84A, Chapter 84B, Chapter 85A, Chapter 85B, Chapter 85C, Chapter 85D, Chapter 86 and in Chapter 98A, Chapter 98B, Chapter 98C .
Anatomy and Classification
Precise knowledge and mastery of the surgical anatomy of the liver, blood vessels, and biliary channels is essential for performing partial hepatectomy; this is described in detail in Chapter 1B. The liver is divided into sectors that comprise liver segments, each supplied by branches of the portal triads and drained by hepatic veins. Partial hepatectomy involves removal of one or more segments by isolation of the relevant portal pedicle, severance of the relevant hepatic veins and biliary drainage channels, and removal of the associated liver tissue.
The anatomic division between the right and left liver is not at the falciform ligament, but rather follows a line projected through a plane—the principal plane or Cantlie’s line—running from the medial margin of the gallbladder bed to the left of the IVC posteriorly (Fig. 90B.2; Couinaud, 1954, 1957; Goldsmith & Woodburne, 1957; Healey & Schroy, 1953; McIndoe & Counseller, 1927). Each of these major right and left portions of the liver is divided into sectors and segments.
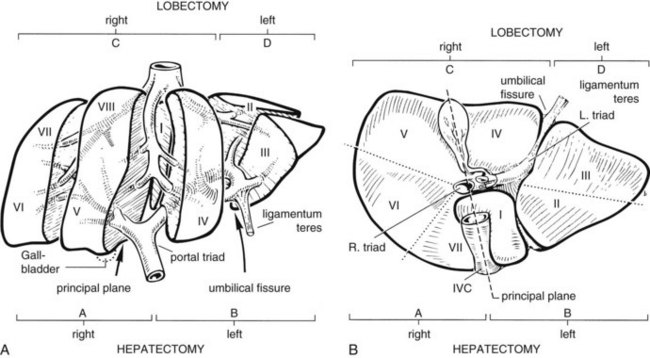
The Brisbane terminology dictates that the hepatic veins form the boundaries between the various sectors of the liver (Strasberg et al, 2000). Specifically, the medial margin of the right posterior sector is the right hepatic vein and comprises segments VI and VII. The right anterior sector is bordered by the right hepatic vein and middle hepatic vein, coursing along the principal plane, and it comprises segments V and VIII. Based on the Brisbane terminology, the area of liver that comprises segments IVa, IVb, and III forms the left medial sector; segment II forms the left lateral sector, because the left hepatic vein actually divides segment II from III. From a clinical perspective, resections of segments III, IVa, and IVb are rarely performed; furthermore, segment IVa/b is often referred to as the left medial sector, or the left medial section in Brisbane terminology, and it is bordered by the middle hepatic vein and umbilical fissure. The left lateral sector, or section, is comprised of segments II and III and represents the portion of liver to the left of the ligamentum teres and falciform ligament; thus in essence, the left liver is divided into a medial and lateral sector along the line of insertion of the ligamentum teres and the falciform ligament. This is the terminology that will be utilized for the remainder of this chapter. The portal venous and hepatic arterial branches conform to the segmental organization and run within the segments, and the draining hepatic veins converge posteriorly toward the inferior vena cava and mark the main scissurae of the liver (see Fig. 90B.2), within which they run (Couinaud, 1954, 1957).
Practically speaking, five types of major anatomic resections are practiced (Fig. 90B.3; see also Fig. 90B.2). The nomenclature of these operations is based on the anatomic descriptions of Couinaud (1954, 1957) and of Bismuth (1982; Table 90B.1). This classification emphasizes the importance of the scissurae of the liver and the umbilical fissure. The alternative, more commonly used terminology of Goldsmith and Woodburne (1957) is also listed in Table 90B.1. A newer terminology proposed by the International Hepato-Pancreatico-Biliary Association in Brisbane (Strasberg et al, 2000) is also referred to in Chapter 1A, Chapter 1B and is discussed above. The five different resections depicted in Figure 90B.3 can also be referred to as 1) right hepatectomy, 2) left hepatectomy, 3) extended right hepatectomy, 4) left lateral sectorectomy, and 5) extended left hepatectomy.
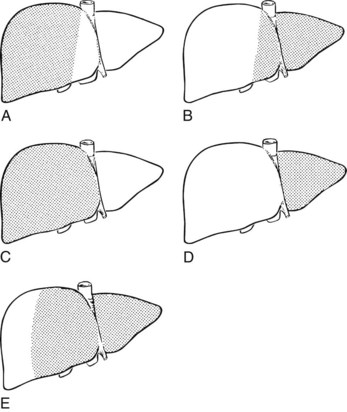
FIGURE 90B.3 Commonly performed major hepatic resections are indicated by shaded areas. A, Right hepatectomy. B, Left hepatectomy. C, Right lobectomy. D, Left lobectomy. E, Extended left hepatectomy. For the nomenclature of Goldsmith and Woodburne (1957), see Table 90B-1.
Table 90B.1 Nomenclature of Hepatic Resection
| Couinaud (1957) | Goldsmith & Woodburne (1957) |
|---|---|
| Right hepatectomy (segments V, VI, VII, VIII; see Fig. 90B.3A) | Right hepatic lobectomy |
| Left hepatectomy (segments II, III, IV; see Fig. 90B.3B) | Left hepatic lobectomy |
| Right lobectomy (segments IV, V, VI, VII, VIII; sometimes includes segment I; see Fig. 90B.3C) | Extended right hepatic lobectomy* |
| Left lobectomy (segments II and III; see Fig. 90B.3D) | Left lateral segmentectomy |
| Extended left hepatectomy (segments II, III, IV, V, VIII; sometimes also segment I†; see Fig. 90B.3E) | Extended left lobectomy† |
* Right lobectomy (extended right hepatic lobectomy) represents right hepatectomy extended to segment IV and has been referred to by Starzl and colleagues (1975, 1980) as right trisegmentectomy; this term is commonly found in the literature.
† Also referred to as left trisegmentectomy (Starzl et al, 1982).
The portal vein and hepatic artery divide into major right and left branches outside the liver substance below the hilus (see Fig. 90B.2A). Here, when the overlying peritoneum is incised, it is possible to dissect each major branch beyond its bifurcation. The confluence of the right and left hepatic ducts also occurs outside the liver. At the hilum of the portal vein, the right branch is short, and its first branch often arises posteroinferiorly, close to the bifurcation, where it is easily damaged during dissection. By contrast, the left branch of the portal vein and the left hepatic duct pursue a longer, more horizontal extrahepatic course beneath segment IV and are more easily dissected free along their length.
The ligamentum teres (round ligament) runs sharply into the umbilical fissure of the liver, at the base of which the main vascular and biliary pedicle branches to the segments of the left liver (II, III, IVa, IVb). After entering the umbilical fissure, the left branch of the portal vein curves caudally and gives branches not only to the left lateral sector, segments II and III, but together with branches of the left hepatic artery, it gives rise to feedback vessels to the left medial sector—segment IVa and IVb of the left liver, also known as the quadrate lobe (see Fig. 90B.2A; Goldsmith & Woodburne, 1957; Starzl et al, 1975).
Outside of the liver substance, there is not a distinct sheath around the portal triad structures, and they must be dissected independently. The structures of the portal triad—the portal vein, hepatic artery, and bile duct—are covered with the Glisson capsule as they enter the liver parenchyma such that within the liver, they are contained in well-formed branching fibrous sheaths often referred to as pedicles. Thus, dissection outside of the liver substance mandates individual isolation of each portal triad structure, where there is considerable variation in anatomy. Pedicles are strong structures that contain the constituents of the portal triad, and intrahepatic dissection of these pedicles enables isolation and control of vascular and biliary elements without the need to individually expose each structure (Launois & Jamieson, 1992b).
The liver straddles the IVC immediately below the diaphragm, and the hepatic veins have a short extrahepatic course to empty into the vena cava (see Fig. 90B.2). This superior portion of the vena cava with the draining hepatic veins is masked behind a fold of peritoneum that extends from the cephalad aspect of the falciform ligament to the right and left triangular ligaments. The right hepatic vein emerges from the right scissura and usually enters the vena cava separately. By contrast, the left hepatic vein, which runs in the left scissura between segments II and III, is often joined by the middle hepatic vein, which occupies the principal scissura, before entering the vena cava. Several smaller veins from the posterior surface of the liver and the caudate lobe drain directly into the IVC.
An additional but important hepatic vein, the umbilical vein, runs beneath the falciform ligament and empties into the left hepatic vein. This vein is important in resections that remove segment IVa, because it provides drainage of segment IVb in the presence of ligation of the middle hepatic vein (see Chapter 92).
Preoperative Considerations
Preoperative Investigations
Preoperative investigations should seek to determine the nature of the lesion and give an index of resectability and the ideal surgical approach. Preoperative transcutaneous needle biopsy of liver tumor masses is not routinely necessary and is not always advisable (see Chapter 20). Preoperative biopsy should be pursued only if the information gained will alter the treatment plan. In the presence of a strong presumptive and clinical diagnosis of a potentially resectable liver tumor, we prefer to avoid the possibility of tumor dissemination, rupture, or hemorrhage, which may occur using percutaneous methods (Thompson et al, 1985). Laparoscopic exploration and visualization, particularly when used in combination with laparoscopic US, may provide valuable information regarding the presence of additional lesions not appreciated on preoperative imaging, and it may also reveal the presence of extrahepatic disease. By minimizing unnecessary laparotomy, this approach has been shown to increase the resectability rate of patients submitted to laparotomy (Jarnagin et al, 2000; John et al, 1994; Li Destri et al, 2008).
There are three major risks of hepatic resection: 1) hemorrhage, which may arise at the porta hepatis from branches of the hepatic artery or portal vein or posteriorly from hepatic venous radicles or the IVC; 2) biliary fistula or stricture as a result of damage to the biliary apparatus; and 3) postoperative liver insufficiency or failure. Intraoperative bleeding complications are most likely to occur when resecting tumors or other lesions that are large and in close proximity to the IVC and/or major hepatic veins (Hawkins et al, 2005). Similarly, tumors near the hilus at the confluence of the hepatic ducts and division of major vessels as they enter the liver substance can be challenging to remove. Given the numerous anatomic variations in the vascular and biliary anatomy of the liver, preoperative cross-sectional imaging should be routinely obtained and evaluated for important spatial relationships between tumor and these structures.
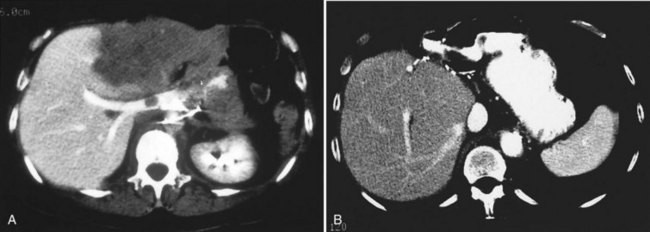
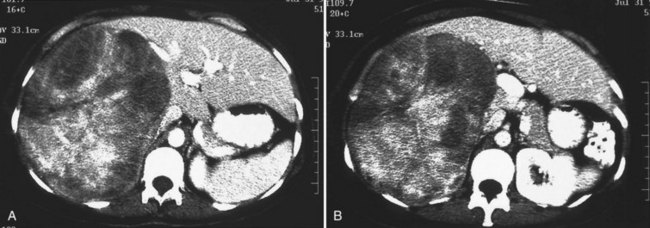
One such modality that provides valuable information in this regard is computed tomography (CT) (see Chapter 16). Peripherally placed lesions, unless substantially large, rarely involve the hilar structures or vena cava; however, more centrally situated lesions may involve major vessels close to the hilus, and appropriate CT scanning (see Chapter 16) can be most helpful in creating an image of the extent of disease and degree of vascular compromise by the tumor (Fig. 90B.4). Liver tumors can sometimes respect intersegmental planes and push structures away rather than invade them directly. This can be demonstrated not only by CT scan (Figs. 90B.5 and 90B.6), but also can be confirmed by angiographic methods (see Fig. 90B.1) or by duplex ultrasound (US). However, with the advancement in technology and the high-quality images obtained with cross-sectional imaging, direct angiography is rarely necessary. Other tumors may hang from the liver in a pedunculated fashion (Baer et al, 1989), and they may be attached to the liver by a relatively small base, even when very large. Such “hanging” tumors are readily depicted on CT scan (Fig. 90B.7). Tumor involvement of the diaphragm also may be suggested by CT, but likewise, this should not deter the surgeon from attempted resection, because such apparent diaphragmatic involvement from metastatic tumors is frequently secondary to an adhesion to a site of previous necrosis of the tumor and not actually from direct tumor invasion (Weinbren & Blumgart, 1986). Primary tumors may still be approached for resection as well, even if they involve the diaphragm (Foster & Berman, 1977).

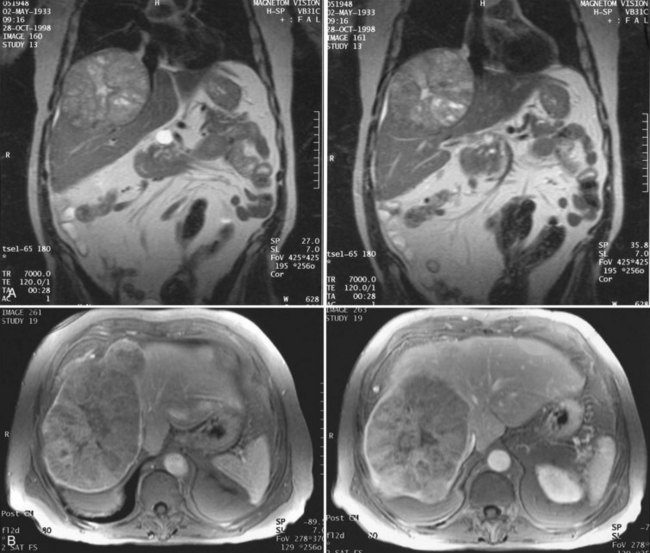
Magnetic resonance imaging (MRI; see Chapter 17) has become increasingly valuable in the imaging of the liver before resection. Masses are well characterized, as are the presence of additional lesions sometimes not visualized on CT scan. MRI depicts major blood vessels accurately and is particularly valuable in the demonstration of the major hepatic veins and vena cava and their relationship to tumor masses (Fig. 90B.8). Compared to CT, MRI also may be more accurate in differentiating primary and secondary malignancies of the liver from benign lesions such as adenoma, focal nodular hyperplasia (FNH), or cysts.
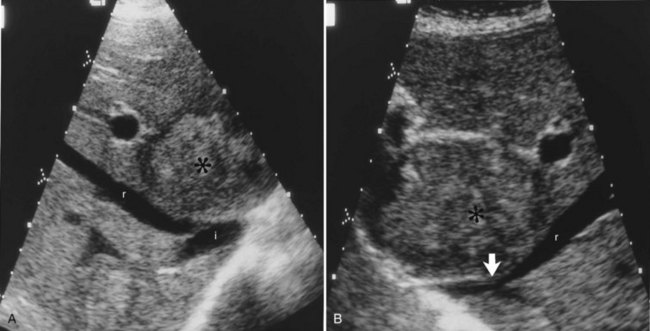
US performed by an experienced operator is also of value in the preoperative assessment of multiple tumors, as it gives information regarding the size of the tumor and extent of liver involvement. US also may help distinguish cysts from solid tumors, and duplex US demonstrates tumor location with respect to important vascular structures, including the hepatic veins and vena cava (Gibson et al, 1986), and it is a valuable technique to further define blood vessels after initial CT scanning (Fig. 90B.9; Hann et al, 1998). US can be of particular importance in the preoperative evaluation of hilar cholangiocarcinoma by defining the extent of involvement of the portal vein and hepatic artery (Fig. 90B.10; Hann et al, 1997); however, as MRI and CT scan continue to produce higher quality images, the need for preoperative US evaluation has declined.

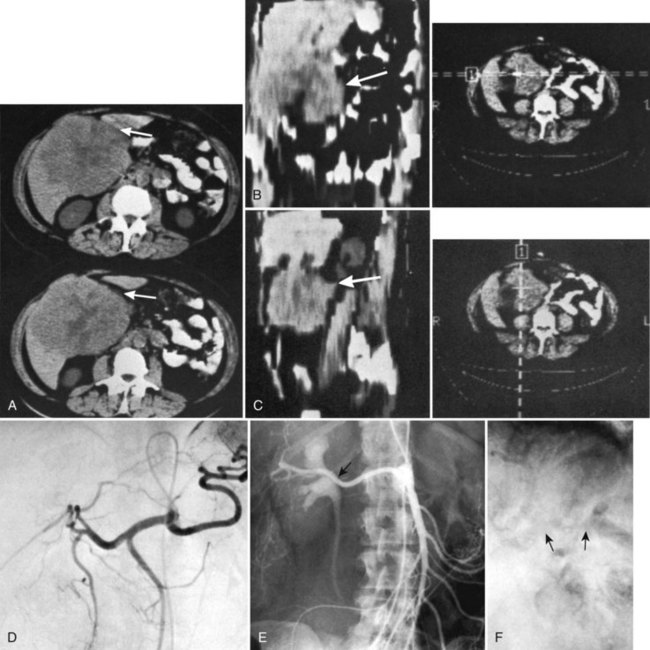
Hepatic angiography and inferior venacavography (see Chapter 19) usually are not necessary and should not be used except perhaps in the instance of large hemangiomata, for which precise information as to the arterial supply of the lesion may assist at surgery, although modern advances in MRI and duplex US have all but rendered these studies obsolete. In the event that adequate US or MRI is unavailable, angiography still has a role in imaging (Blumgart, 1982; Voyles et al, 1983). Some figures of angiographic techniques are provided for illustrative purposes (Fig. 90B.11; see also Figs. 90B.1 and 90B.7), but it should be emphasized that they are unnecessary in most patients. In our practice, hepatic angiography is rarely obtained for the preoperative demonstration of extrahepatic arterial anatomy in patients being considered for placement of a hepatic arterial infusion (HAI) pump for postoperative adjunctive chemotherapy (see Chapter 86).

Other Investigations
To determine the oncologic appropriateness of hepatic resection, a thorough evaluation for the presence of extrahepatic disease should be performed by means of chest radiography, CT, or MRI before major hepatic resection is undertaken. When evaluating the chest, subcentimeter pulmonary nodules are frequently encountered that should not necessarily preclude hepatic resection, particularly for colorectal cancer liver metastases (Maithel et al, 2010). Positron-emission tomography (PET) scan may also be an important tool in the evaluation of the extent of spread of malignant disease (see Chapter 15; Beets et al, 1994; Fong et al, 1999a; Lai et al, 1996; Schüssler-Fiorenza et al, 2004).
If jaundice is present, and biliary involvement by the tumor is suspected, direct cholangiography may be carried out, either by endoscopic retrograde cholangiography (ERCP) or by percutaneous transhepatic cholangiography, to delineate the biliary anatomy (see Chapter 18); however, US and MRI cholangiography are noninvasive studies in many ways superior to direct cholangiography, and they have all but replaced preoperative invasive cholangiography for assessing tumor involvement of the bile ducts, such as in hilar cholangiocarcinoma (see Fig. 90B.10; see also Chapter 52). Of course, if preoperative biliary drainage is necessary, direct cholangiography, either endoscopic or percutaneous, will be required.
Staging Laparoscopy
Staging laparoscopy and laparoscopic US are widely used to prevent unnecessary laparotomy in patients with hepatobiliary malignancy. Staging laparoscopy can significantly improve resectability rates at laparotomy, and laparoscopic evaluation has its greatest yield in detecting peritoneal metastases not detectable on cross-sectional imaging rather than identifying additional hepatic lesions. Furthermore, because of their location, laparoscopic evaluation often fails to identify lymph node metastases (Jarnagin et al, 2000; John et al, 1994; Lo et al, 1998). In one study at MSKCC (Jarnagin et al, 2000), 83% of patients subjected to laparotomy after laparoscopy underwent potentially curative resection, compared with only 66% of patients not staged laparoscopically (see Chapter 21).
Assessment of Resectability
Major difficulties with accurate preoperative assessment of resectability can arise in two situations: First, tumors situated near the major hilar structures (see Fig. 90B.7) or those markedly compressing (see Fig. 90B.11) or involving the vena cava can be difficult to assess preoperatively. Involvement of major structures, such as invasion of bile ducts or portal venous branches, or apparent involvement of the IVC does not necessarily preclude resection (see Fig. 90B.1; Soreide et al, 1985). Second, very large tumors, which push structures aside and have been slowly growing over a long time, are difficult to define precisely, because pressure changes may mimic invasion on radiologic images. Thus, considerable caution must be exercised before declaring such cases unresectable. In patients with tumors of this nature, it is often difficult at initial exploration to be certain of resectability, and considerable dissection and mobilization is necessary before a clear-cut decision can be made. The morphologic configuration of tumors on imaging studies has been shown to have a clear relationship to subsequent resectability. Tumors that expand and compress surrounding tissues (pushing tumors) and tumors that are pedunculated and attached to the liver by a base of narrow width (hanging tumors) are nearly always resectable, and they can be distinguished from tumors that are irregular at the margins and clearly invasive (Baer et al, 1989).
In the early years of hepatic resection, the editor emeritus (Leslie H. Blumgart) adopted and promoted a deliberate policy of full investigation at laparotomy to assess resectability in all patients with solitary large liver tumors, provided no positive evidence of extrahepatic spread was apparent, patients were otherwise fit for major surgery, and the residual liver would be adequate. Of 22 patients with primary liver cancer evaluated in an early study, 13 patients were explored, and resection was carried out in all 13. Only three (23%) of the 13 underwent either a right or left hepatectomy or lesser procedure; the rest were submitted to extensive resections crossing the principal scissura (Cantlie’s line) and necessitated extended resection (see Fig. 90B.11). Two of these 13 patients had tumor embolization before surgery to reduce vascularity and tumor size. Eight of these tumors were found to involve the right and left liver on CT scan; involvement of the main portal vein by tumor extension was found in two patients, one patient had involvement of the right branch of the portal vein, and six patients had severe compression or involvement of the IVC (see Fig. 90B.11). Although extrahepatic involvement was suspected in 3 patients, the resections carried out were potentially curative in 12 of the 13 patients with macroscopic clearance of all tumor; but in 1 patient with fibrolamellar hepatocellular carcinoma (HCC), a deliberate extended resection was performed in the presence of regional lymph node metastases. No intraoperative or in-hospital (30-day) deaths were reported (Soreide et al, 1985). This early experience has been replicated in subsequent studies (Vauthey et al, 1993) and in studies by many other investigators.
The resectability rate within a specialized hepatobiliary surgery unit does not necessarily indicate the overall resectability rate for a particular tumor, because the patient population is highly selected; however, it does seem that an aggressive surgical policy is justified, even in patients with large solitary tumors. In particular, the size of the tumor alone is not a contraindication to resection, although for HCC, large tumor size is associated with earlier recurrence and reduced survival (Pawlik et al, 2005; Nathan et al, 2009). Other authors agree with this view and advocate an aggressive approach to resection (Adson & Weiland, 1981; Balasegaram & Joishy, 1981; Okamoto et al, 1984; Starzl et al, 1982
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
 Portal hypertension in children
Portal hypertension in children
 Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
 Bile duct exploration and biliary-enteric anastomosis
Bile duct exploration and biliary-enteric anastomosis
 Recurrent pyogenic cholangitis
Recurrent pyogenic cholangitis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


