Fig. 23.1
Operating room set-up. (a) Operator, (b) assistant, (c) nurse
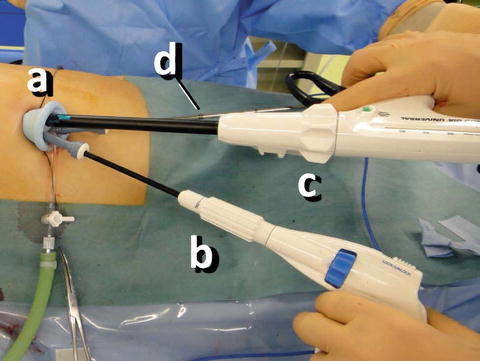
Fig. 23.2
Access through the umbilicus. (a) SILS Port™ (Covidien), (b) articulating grasper, (c) linear stapler, (d) 5-mm flexible scope (behind the scope)
23.4 S-DP Without Splenic Preservation
The first step is dissection of the ligamentous attachments around the spleen for its mobilization. A 5-mm LigaSure V (Valleylab; Covidien) is used for the dissection of all ligaments as well as small vessels such as the short gastric vessels. By dissecting the gastrocolic and gastrosplenic ligaments, the omental bursa is opened toward the superior pole of the spleen, and the splenic hilum is well exposed. The inferior pole of the spleen is then freed by dissecting the splenocolic ligament. The phrenosplenic ligament is also dissected. After dissection of both the superior and inferior poles of the spleen, the retroperitoneum lateral to the spleen (the splenorenal ligament) is dissected toward the superior pole of the spleen. After rough completion of splenic hilar dissection, one of the three 5-mm trocars is temporarily replaced by a 12-mm trocar, through which a 3- to 5-mm width cloth tape is introduced intraperitoneally to encircle and tug the splenic hilum. Both ends of the tape are grasped and exteriorized with the use of a laparoscopic suture passer or mini-loop retractor (Mini Loop Retractor II; Hakkou-shoji, Tokyo, Japan) through a needle hole that is approximately 2 mm in diameter and placed on the left midaxillary line 1 cm inferior to the costal margin (Fig. 23.3a, b). By pulling the tape with the use of an extracorporeal clamp or laparoscopic graspers in appropriate directions, excellent exposure of the splenic hilum and the pancreatic tail is obtained. This method is known as the tug-exposure technique [10]. This technique is also helpful for dissecting the remnant ligaments around the spleen and for detaching the pancreas, tail to body, from the retroperitoneum. Another 5-mm trocar is replaced by a 12-mm trocar that allows introduction of an endostapler (60 mm in length, 4.8-mm staples; Covidien). Although we have reported use of a six-row stapler to prevent postoperative pancreatic fistula, the six-row stapler does not have an articulating function for closing the pancreatic stump in LDP [18]. The articulating function of the linear stapler is indispensable; it ensures an optimal angle in transecting the pancreatic parenchyma. The pancreas, together with the splenic vessels, is divided with the stapler. If minor bleeding from the arterial stump occurs, application of a metal clip is effective. If there is any oozing from the parenchymal stump, argon beam coagulation is useful. The12-mm trocar is then temporarily removed, and an EndoCatch II retrieval bag (Covidien) is introduced directly through a channel of the SILS™ Port. In the case of a cystic tumor, the fluid content is aspirated within the retrieval bag by direct puncture with an 18G needle through the umbilical wound; careful attention must be paid to avoid spillage. Then, through the umbilical wound, the spleen is pierced with Péan forceps to suction an aliquot of blood into the bag. These techniques facilitate extraction of the specimen through the umbilical wound without any need to extend the skin incision (Fig. 23.4a, b). A small silicone drain is placed in the splenic fossa, and the drain tube is extracted from the bottom of the umbilicus. Finally the umbilical wound is closed, with 0-Vicryl used for the fascia and 5-0 PDS used for subcutaneous suture.
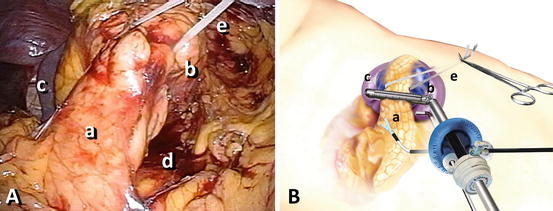
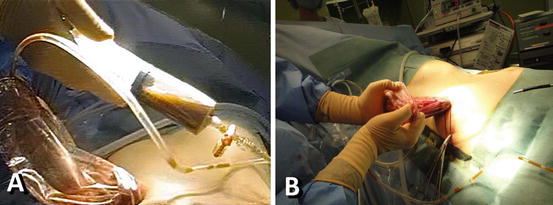
Fig. 23.3
Photograph of an actual SLS-DP (a) and an illustration of SLS-DP (b) in which the tug-exposure technique is used for a large cystic tumor in the pancreatic tail. The pancreas is mobilized, tail to body, and lifted from the retroperitoneum with a cloth tape. (a) pancreas, (b) cystic tumor, (c) spleen, (d) retroperitoneal space, (e) cloth tape
Fig. 23.4
The cystic contents are aspirated within the retrieval bag (a). Extraction of the pancreatic tail, the cyst, and the spleen from the umbilical wound (b)
23.5 SLS-DP with Splenic Preservation
The greater curvature of the stomach is suspended with two sutures of 2-0 Ethibond Excel (Ethicon, Cincinnati, OH, USA), which provides excellent exposure of the pancreas from body to tail and of the tumor behind the stomach after the omentum is opened (Fig. 23.5). This technique is applicable to any SLS-pancreatectomy including the SLS-DP described above. The tail of the pancreas is then carefully detached from the retroperitoneum and the splenic vessels. Careful attention should be paid to the treatment of the branches of the splenic vein and artery. A 5-mm LigaSure™V with a dolphin tip is useful for sealing and cutting the small branches. A balloon-type retractor (Cat Hand; Hakko Co., Nagano, Japan) provides excellent exposure by gentle retraction of the pancreas during the dissection. When the splenic artery and vein, and sometimes the inferior mesenteric vein, are well freed and exposed (Fig. 23.6), the pancreatic parenchyma is divided with use of the endostapler (60 mm in length, 4.8-mm staples; (Covidien) as performed in S-DP without splenic preservation. The resected specimen is extracted through the umbilical site in a retrieval bag. A small silicone drain is placed in the splenic fossa through the umbilical wound, which is closed in the same manner as described above. The umbilical wound is nearly invisible 1 month after surgery (Fig. 23.7).
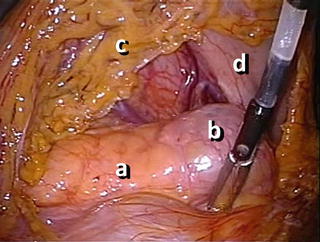
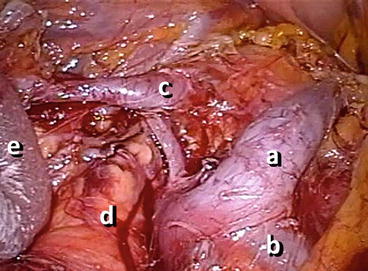

Fig. 23.5
The pancreas and the tumor behind the stomach are well visualized after the omentum is opened. The greater curvature of the stomach is suspended by two sutures. (a) Pancreas, (b) tumor, (c) omentum, (d) stomach
Fig. 23.6
The splenic vein (a), inferior mesenteric vein (b), and splenic artery (c) are well visualized behind the pancreas (d), which is retracted toward the right side with a balloon retractor (e)
Fig. 23.7




The umbilical wound is almost invisible 1 month after surgery
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
