Chapter 42B Biliary fistulae
Internal Biliary Fistulae
Incidence and Etiology
Whether occurring as a consequence of calculous biliary tract disease, trauma, neoplasm, or congenital anomalies, internal biliary fistulae are uncommon. Estimates of incidence are crude, gleaned only from many small series, usually with fewer than 50 patients. If all types of internal biliary fistula are included, calculous biliary tract disease accounts for 90%; peptic ulcer disease, 6%; and neoplasm, trauma, parasitic infection, and congenital anomalies make up the remaining 4% (Piedad & Wels, 1972).
Overall, 1% to 3% of patients with cholesterol cholethiasis in Western countries develop biliary-enteric fistula, with a female/male ratio of 3 : 1. In 11,808 cases of nonmalignant biliary tract disease encountered at New York Hospital/Cornell Medical Center during the years 1932 through 1978, the incidence of biliary-enteric fistula was 0.9% with a male/female ratio of 2.3 : 1 (Glenn et al, 1981). A large series from Greece (Lygidakis, 1981) showed an incidence of 2%, and in Native Americans, the incidence is 3.2% (Zwemer et al, 1979). In Japan, where bilirubin stones and primary intraductal disease predominate, the incidence of fistula is between 13% and 18% with a slight male predominance (Urakami & Kishi, 1978). The type of fistula noted in this group of patients usually involves the ductal system rather than the gallbladder. The pathogenic sequence of events for calculous biliary tract disease has been well described by Glenn and Mannix (1957). It consists of pressure necrosis and erosion of part of the biliary tract wall into an adjacent structure to which it has become adherent in the course of repeated bouts of inflammation, often with distal biliary tract obstruction. The likelihood of the branches of the hepatobiliary tree to become inflamed and anatomic proximity to adjacent hollow viscera largely determine the relative incidence of the different types of spontaneous biliary-enteric fistulae secondary to calculous disease.
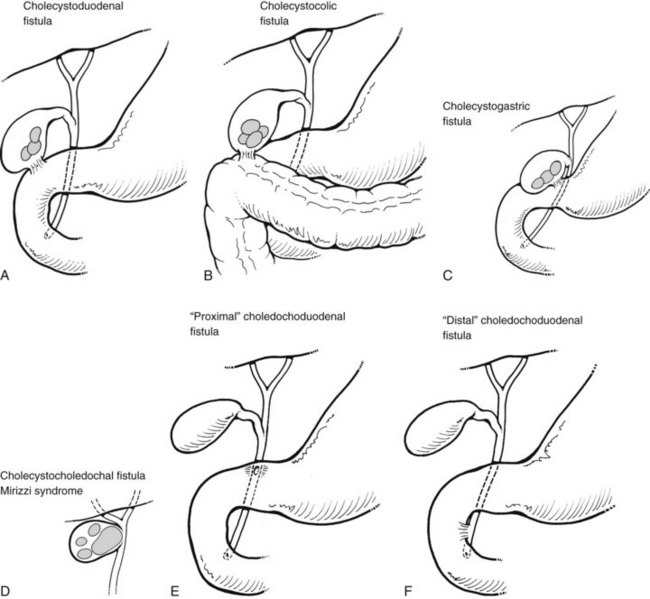
The various types of biliary-enteric fistulae can best be subclassified from an anatomic point of view, by the names of the principal organs involved (Fig. 42B.1). Some names for a particular fistula between two structures vary in the literature (e.g., bronchobiliary vs. biliobronchial) but do not connote differences in etiology or pathogenesis.
Fistulae Involving the Gallbladder
In Western countries, where cholesterol cholelithiasis abounds, the gallbladder is most often the site of severe inflammation and obstruction. Cholecystenteric fistulae constitute 70% to 85% of all biliary fistulae reported in the world literature up to 1982 (Rau et al, 1980; Safaie-Shirazi et al, 1973). Of these, 55% to 75% are cholecystoduodenal, 15% to 30% are cholecystocolic, and 2% to 5% are cholecystogastric (see Fig. 42B.1). Multiple fistulae (e.g., cholecystoduodenocolic) are very rare (Shocket et al, 1970). Of the 23 cases reported up to 1978, 21 were secondary to gallstone disease, and one case of each was due to duodenal ulcer and a primary carcinoma of the gallbladder (Morris et al, 1978).
Gallstone ileus, a dramatic clinical presentation of a cholecystenteric fistula, is reported in 8% to 20% of large series of patients with biliary-enteric fistulae (Clavien et al, 1990; Heuman et al, 1980; Kasahara et al, 1980; LeBlanc et al, 1983; Rau et al, 1980; Safaie-Shirazi et al, 1973; VanLandingham & Broders, 1982). As a cause of intestinal obstruction alone, gallstone ileus accounts for 1% to 4% of cases, although in patients older than 65 years, gallstone ileus may account for 25% of cases of small bowel obstruction, regardless of a history of prior abdominal surgery (Clavien et al, 1990; Reisner & Cohen, 1994; Rodriguez-Hermosa et al, 2001; Lassandro et al, 2004; Kirchmayr et al, 2005; Chou et al, 2007).
Although most fistulae between the gallbladder and intestinal tract become obvious preoperatively or intraoperatively, cholecystocholedochal fistulae are insidious and may not be appreciated even at surgery. These biliobiliary fistulae develop between the ampulla of the gallbladder or cystic duct and the proximal common hepatic or common bile duct (CBD; see Fig. 42B.1D). In either instance, the mechanism of formation is the same: pressure necrosis into the common duct by a large solitary calculus impacted in either the ampulla of the gallbladder or the intramural portion of the cystic duct. Cholecystocholedochal fistula has been estimated to occur in 1% to 6% of biliary operations for calculous disease (Corlette & Bismuth, 1975). Although this estimate seems high and is not corroborated by other reports, an awareness of the possibility of cholecystocholedochal fistula is important and may help avoid damage to the common duct at operation.
Fistulae Involving the Common Bile Duct, Cystic Duct Remnant, and Other Extrahepatic Ducts
Choledochoduodenal fistulae are classified as either proximal or distal (see Fig. 42B.1E and 42B.1F). A proximal choledochoduodenal fistula is the principal form of abnormal communication between the CBD and adjacent structures and represents 4% to 20% of all biliary-enteric fistulae. At one time, 80% were caused by peptic ulcer erosion from the first portion of the duodenum into the proximal CBD. This cause is now much less common as a result of the development of effective medical therapy with antacid drugs. Other, less common causes of choledochoduodenal fistula include cholelithiasis, operative trauma, duodenal diverticula, echinococcal infection, Crohn disease, and neoplasms of the stomach, distal bile duct, ampullary region, and duodenum (Feller et al, 1980; Sarr et al, 1981; Kuroki et al, 2005). Since the beginning of the acquired immunodeficiency syndrome (AIDS) epidemic, there have only been three known case reports of choledochoduodenal fistula caused by AIDS/human immunodeficiency virus–associated tuberculous infection (Patino et al, 2003).
Distal choledochoduodenal fistulae connect to the duodenum in the distal 2 cm of the CBD, and the fistula opening can be seen during percutaneous transhepatic cholangiography (PTC) and endoscopic retrograde cholangiopancreatography (ERCP). The incidence of distal choledochoduodenal fistula secondary to cholelithiasis or operative trauma is variable in different parts of the world. With the development of PTC and ERCP studies of pathologic anatomy (see Chapters 18, 27, and 28), it is becoming apparent that many patients with minor or major biliary-digestive complaints and gallstone disease may have a distal choledochoduodenal or parapapillary choledochoduodenal fistula. Large series from Argentina showed the incidence of parapapillary choledochoduodenal fistula to be 0.7%. Jorge and colleagues (1991) reviewed 2012 ERCP studies from 1976 through 1989, and only 14 cases were found: two cases were from stone disease and the other 12 were from iatrogenic causes.
In Japan, where there is a high incidence of primary intrahepatic calculous biliary tract disease, Tanaka and Ikeda (1983) reported a 5.3% incidence of parapapillary fistula in ERCP studies of 1500 patients. The male/female ratio was roughly equal, in keeping with the Japanese sex distribution of gallstone disease. Ikeda and Okada (1975) classified these as type I fistula, characterized by a small fistula opening on the longitudinal fold of the duodenum just proximal to the papilla, probably caused by penetration of a small calculus through the intramural portion of the common duct into the duodenum, and type II fistula, a larger opening of the duodenum wall adjacent to the longitudinal fold, probably caused by a relatively large stone eroding from the extramural portion of a greatly dilated common duct into the duodenum.
In Turkey, Karincaoglu and colleagues (2003a) reported an incidence rate of 4.9% on review of 1347 ERCP studies in 841 patients. This study also found an intriguing association between peripapillary fistula with common duct stones and complications of cholangitis. The incidence of parapapillary choledochoduodenal fistula is probably less in Western Europe, the United Kingdom, and the United States, and perhaps a greater proportion of these fistulae are not due to spontaneous gallstone disease itself but rather to iatrogenic surgical injury or other instrumental damage to the distal common duct in operations directed against choledocholithiasis. Hunt and Blumgart (1980) and Tytgat and colleagues (1979) published their experience of these fistulous complications of biliary tract surgery.
Unusual choledochal fistulae are mentioned only briefly in this context. Spontaneous fistula formation between the common duct and the colon has been recorded only four times in the English literature (Bose & Sastry, 1983; Rawas et al, 1987; Guitron-Cantu et al, 2001; Anees et al, 2008). We are also aware of one case of a choledochocolonic fistula that developed after blunt abdominal trauma (Benson et al, 2001) and another that developed as a complication from diverticulitis (Blanco-Benavides & Rodriguez-Jerkov, 1992). Peptic ulcer disease has rarely produced fistulae between the common duct, duodenum, and pancreas (Aitken et al, 1986). We have observed one case and are aware of several other cases of severe pancreatitis or pancreatic cancer producing a fistulous communication between pancreatic pseudocysts or necrotic pancreatic cavities and the CBD (DeVanna et al, 1983; Ellenbogen et al, 1981; Lebovics et al, 1990; Miller et al, 1988). Chandar and Hookman (1980) reported one case of GI hemorrhage resulting from a choledochocolonic fistula that developed from a cystic duct remnant 28 years after cholecystectomy, and it was associated with a benign stricture in the ampullary segment of the CBD. More recently, a bile duct stricture associated with a choledochocolonic fistula was reported following an uncomplicated open cholecystectomy four months prior (Munene et al, 2006). Woods and colleagues (1992) reviewed four cases of cystic duct remnant fistulization to the GI tract.
Fistulae Involving the Intrahepatic Ducts, Liver, and Lung
Thoracobiliary and bronchobiliary fistulae are quite rare (Boyd, 1977; Chan et al, 1984; Cleve & Correa, 1958); the former refers to communications between the biliary tree and the pleural cavity and the latter to communications between the bile ducts and the bronchial tree. The three major categories of bronchobiliary fistula are 1) those resulting from infection, especially parasitic, or those acquired, such as from iatrogenic injury as a result of biliary tract surgery or, less commonly, from gastric and pancreatic operations; 2) traumatic fistula; and 3) congenital fistula. The many diverse causes of acquired bronchobiliary fistulae have been well referenced by Sane and colleagues (1971) and more recently by Gugenheim and colleagues (1988). The two main factors responsible for the development of bronchobiliary fistulas are “mechanical” biliary obstruction and infection. Worldwide, the principal cause of bronchobiliary fistula in adults is parasitic disease of the liver, either echinococcal or amebic abscess (see Chapters 67 and 68). In developed countries, iatrogenic injury to the biliary ductal system is the most frequent cause of these fistulae.
The hallmark symptom of a bronchobiliary fistula is biliptysis in conjunction with other pulmonary complaints, jaundice, cholangitis, and external biliary fistula or subphrenic abscess. Radiologic confirmation of the diagnosis is possible by a variety of methods. In the presence of an external fistula, injection of contrast solution (fistulogram) is the most facile and direct approach. PTC and ERCP are equally effective in their ability to show the fistula and have the advantage of offering an avenue for potential therapeutic intervention. The choice of one or the other of these techniques depends on the presence or absence of dilated ducts and the expertise available. Bronchobiliary fistulae also have been shown by cholescintigraphy (Gunlemez et al, 2009; Santra et al, 2009; Uramoto et al, 2008; Andalkar et al, 2004; Savitch et al, 1983; Velchik et al, 1991). Computed tomography (CT) and magnetic resonance imaging cholangiopancreatography (MRCP) have been used to assess bronchobiliary fistulae (see Chapters 16 and 17). These imaging techniques, although helpful in assessing the upper abdomen, rarely visualize the fistula tract (Oettl et al, 1999; Yeatman et al, 2004; Kuroki et al, 2005; Ragozzino et al, 2005).
The surgical treatment of parasitic disease of the liver is discussed elsewhere in this book (see Chapters 67 and 68). In large series of surgically treated cases of hepatic echinococcal disease in Greece and Turkey, only 2% were complicated by rupture into the lung or bronchi (Alestig et al, 1972). Amebic abscess of the liver has been reported in association with bronchobiliary fistula in 8% of cases (Razemon et al, 1963). These complications of parasitic disease are more likely to be suspected in patients from Mediterranean countries, North Africa, Mexico, and some of the southern border states of the United States. The successful treatment of these fistulae depends on the use of appropriate surgical drainage or resection in conjunction with appropriate drug therapy.
The incidence of bronchobiliary fistula as a consequence of surgically treated calculous or neoplastic disease of the hepatobiliary tract and adjacent structures has been decreasing, as patients are operated on earlier in the course of their disease and by better-trained surgeons (Ramesh et al, 1991; Warren et al, 1983). Then again, modern surgical techniques and equipment have contributed to a new cause of biliary fistulae: reports of bronchobiliary fistula caused by new liver tumor ablative therapies, such as radiofrequency ablation (RFA), are beginning to emerge (Kim et al, 2005; Tran et al, 2007; Yoon et al, 2009; see Chapter 85A, Chapter 85B, Chapter 85C, Chapter 85D ). In all these case reports, the fistula responded to conservative treatments focused on biliary drainage.
The incidence of bile duct injury in the course of cholecystectomy has increased with the advent of laparoscopic removal of the calculous gallbladder (Davidoff et al, 1992). Most of the injuries are repaired at or shortly after their occurrence. Bronchobiliary fistulae secondary to bile duct injury are a late consequence of the event in patients with neglected or recurrent strictures after unsuccessful operations. Less frequently, gastric or pancreatic procedures may result in injury to the extrahepatic bile ducts.
Untreated choledocholithiasis complicated by repeated episodes of bile duct obstruction and cholangitis is another, albeit infrequent, cause of bronchobiliary fistula. Brem and colleagues (1990) reported the successful treatment of an 87-year-old patient with this clinical situation by endoscopic papillotomy alone. Indeed, bronchobiliary fistulae should be treated first by biliary decompression, either by endoscopic papillotomy or by transampullary drainage to reduce the fistula tract pressure. Some patients with a persistent fistula or infection will require debridement by thoracotomy.
Posttraumatic thoracobiliary fistulae are extremely rare. Although penetrating or blunt trauma to the abdomen and chest is a common enough civilian and wartime occurrence, the number of fistulae resulting has remained small, often because their initial surgical treatment has been excellent, and because no obstruction to proper bile flow existed (Oparah & Mandal, 1978). Ivatury and colleagues (1984) reported on three cases and reviewed 32 previously reported patients. This series included 20 thoracobiliary and 15 bronchobiliary fistulae. Twenty-six patients sustained penetrating injuries, including 16 with gunshot wounds, 6 with stab wounds, and 4 in which the weapon was not specified. Seven patients were admitted because of blunt trauma, and in an additional four patients, the mechanism of injury was not documented. All of the patients in this report had thoracoabdominal injuries, and the causes of the fistulae were nonoperative therapy, missed or overlooked injury to the diaphragm, inadequate drainage, and subphrenic abscess. All patients had pleural effusion, and bile was aspirated by thoracentesis. Successful treatment frequently required pulmonary decortication, repair of the diaphragm, and adequate drainage above and below the diaphragm. More recent publications support the notion that inadequate drainage caused posttraumatic bronchobiliary fistulae (Navsaria et al, 2002; Eryigit et al, 2007; Ball et al, 2009).
Neuhauser and colleagues (1952) first described congenital bronchobiliary fistula in an infant with a tract communicating between the right main stem bronchus and the hepatic duct that passed through the posterior mediastinum. The diagnosis was made antemortem, but the infant died before surgical therapy. Tommasoni and colleagues (2000) described two newborn infants who were promptly diagnosed and successfully treated surgically. These authors emphasized the importance of a high index of suspicion for early diagnosis and recognition of the very high incidence (approximately 36%) of coexisting hypoplasia or biliary atresia. Therefore, all of these patients need laparotomy and thoracotomy for successful treatment (Tommasoni et al, 2000). The fistulous tract in the posterior mediastinum adjacent to the esophagus should also be excised to avoid repeat thoractomy (Gunlemez et al, 2009). Yamaguchi and colleagues (1990) reported one adult patient with a congenital bronchobiliary fistula and summarized the data of 16 previously reported cases, four of them adults. Interestingly, all adults were younger than 32 years (range, 22 to 32 years). The only congentital bronchobiliary fistula in an elderly person was reported recently by Uramoto (2008).
On microscopic examination, the proximal portion of the fistula in most patients resembles the bronchus, and the distal segment resembles the esophagus; the embryologic explanations for this anomaly are conjectural (Dyon et al, 1978; Sane et al, 1971). Transthoracic excision of the fistula and surgical correction of associated biliary anomolies is usually curative.
Diagnostic Tests
Sputum analysis for bilirubin and viable scolices or membranes can be used as laboratory evidence to establish the diagnosis of bronchobiliary fistulae secondary to echinococcosis (Gerazounis et al, 2002). Although no specific serologic tests for biliary-enteric fistula are available, in the evaluation and management of an elderly, high-risk, or critically ill patient with a symptomatic biliary fistula, tests of liver function, electrolytes, and blood count are useful.
Plain and Contrast Radiographs
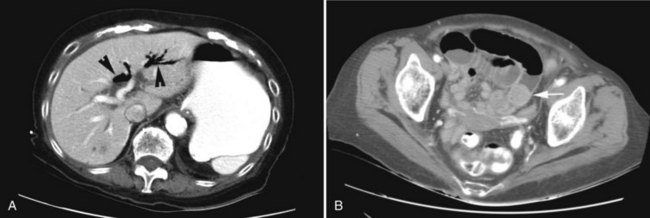
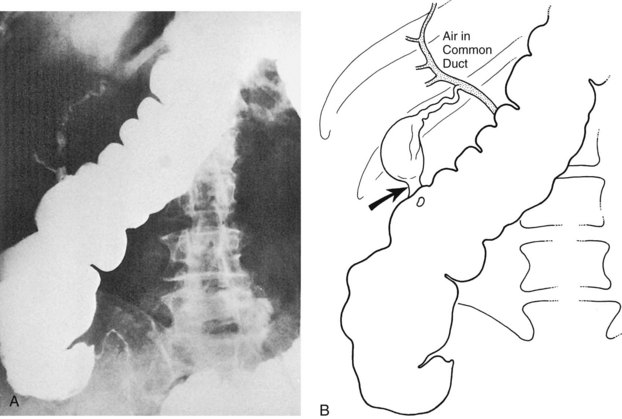
Pneumobilia, the presence of air in the biliary tree, may be noted on plain films of 30% to 50% of patients with gallstone ileus (Fig. 42B.2A). Other, less common causes of pneumobilia include an incompetent sphincter of Oddi, emphysematous cholecystitis, suppurative cholangitis, and prior biliary-enteric bypass surgery. Hricak and Vander Molen (1978) suggested that the low incidence of pneumobilia in gallstone ileus is due to the cystic duct obstruction that led to the acute cholecystitis and perforation into an adjacent viscus; the obstruction also prevents retrograde passage of air into the extrahepatic and intrahepatic bile ducts.

Other classic radiographic signs of gallstone ileus are visualization of a calcified gallstone in the peritoneal cavity a distance away from the gallbladder (Fig. 42B.2B), change on repeat films in the position of a previously observed calcification, and a change in the level of mechanical intestinal obstruction—the so-called tumbling obstruction (Day & Marks, 1975; VanLandingham & Broders, 1982). However, only 30% of gallstones are sufficiently calcified to be radiopaque.
A barium meal or upper GI series shows reflux of contrast material into the fistula in 40% of cholecystoduodenal communications and 75% of choledochoduodenal fistulae of peptic ulcer origin (Balthazar & Gurkin, 1976; Kourias & Chouliaras, 1964). If the plain film and barium swallow are used in concert, more than 60% of biliary enteric fistulae are correctly diagnosed preoperatively (see Fig. 42B.2A; Balthazar & Schechter, 1975). A negative upper GI series in the presence of pneumobilia is an indication for a barium enema, which discloses more than 95% of cholecystocolic fistulae. CT scans with contrast material, endoscopy, radionuclide imaging, and sonography are also useful in the diagnosis of biliary fistulae (Becker et al, 1984); and more recently, MRCP has yielded valuable information.
Endoscopy and Iodinated Dye Studies
Since 1970, numerous reports have appeared in the literature supporting the efficacy of ERCP in documenting surgical or spontaneous biliary fistulae (Al Nakib et al, 1982; Tanaka & Ikeda, 1983; Tytgat et al, 1979; Van Linda & Rosson, 1984). Endoscopically, the alimentary side of a fistula can be visualized directly, be it gastric (Stempfle & Diamantopoulos, 1976), duodenal, or colic; the fistula itself or the ampulla of Vater can be cannulated to obtain a high-quality radiograph of the communicating biliary anatomy (Moreira et al, 1984; Watkins et al, 1975; Chatzoulis et al, 2007). Similarly, the largely unappreciated and frequently asymptomatic parapapillary choledochoduodenal fistula has been found to be quite common (Hunt & Blumgart, 1980; Karincaoglu et al, 2003b; Tanaka & Ikeda, 1983; Kuroki et al, 2005). There have been far fewer reports of the role of PTC in showing biliary fistulae, but PTC has been helpful in the diagnosis and treatment of bronchobiliary fistula in association with echinococcal disease of the liver and dilated intrahepatic ducts (e.g., cholecystocholedochal fistula; Cornud et al, 1981; Mannella et al, 1999).
Radionuclide Imaging (See Chapter 15)
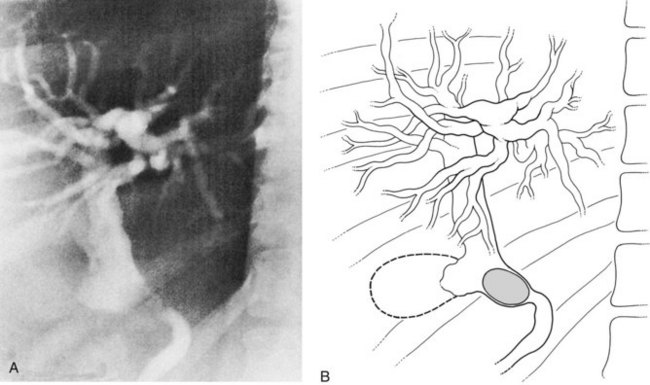
With the introduction of the imidoacetic acid agents bound to technetium (p-isopropylacetanilido iminodiacetic acid [PIPIDA] and hepatobiliary iminodiacetic acid [HIDA]), radionuclide scans have rapidly become the preferred method of outlining the normal and pathologic anatomy of the extrahepatic bile passages. These relatively noninvasive procedures do not rely on hepatocellular concentration of bile or on short critical time-flow periods for satisfactory visualization of the biliary tree. Prolonged (24 hours) accumulation of radioactivity, measured by patient scanning or quantitative isotopic counts of body secretions (e.g., sputum), has been used to show very small or intermittent fistulae from the biliary tract to the respiratory passages (Fig. 42B.3) and the colon (Benson et al, 2001; Santra et al, 2009; Uramoto et al, 2008; Andalkar et al, 2004; Bretland, 1983; Edell et al, 1981; Henderson et al, 1981; Savitch et al, 1983; Taillefer et al, 1983).

Sonography
Sonography is a useful noninvasive diagnostic aid in the preoperative evaluation of a patient with a suspected biliary fistula (Porta et al, 1981; Renner et al, 1982) and even gallstone ileus (Davies et al, 1991; Pedersen et al, 1988; see Chapter 13). Although the radionuclide scan may readily show a fistula, the sonogram indicates the presence of calculi in the gallbladder; common duct stones; and inflammatory, cystic, or infiltrative disease of the liver and pancreas (Griffin et al, 1983). Sonography can readily detect pneumobilia, indicating a high likelihood of a biliary-enteric fistula. In gallstone ileus, sonography can detect an ileal stone not seen on plain films and is increasingly being used by emergency room physicians (Zironi et al, 2007). Ripolles and colleagues (2001) reported that 22 of 23 patients who had undergone surgery for gallstone ileus were found on sonogram to have pneumobilia. This information is valuable in the decision-making process, such as to evaluate the need for or advisability of cholecystectomy and dismantling of a fistula at the time of operation for gallstone ileus in an elderly or high-risk patient. This information may be obtained more rapidly and safely, and probably with equivalent accuracy, by a preoperative sonogram rather than by intraoperative manipulations about the mass of inflamed tissue in the right upper quadrant. Ultrasound (US) has been used to document the persistence or closure of biliary enteric fistulae after initial emergent surgical or combined endoscopic lithotripter treatment of gallstone ileus, and it has aided the decision for or against further surgery (Clavien et al, 1990).
Computed Tomography and Magnetic Resonance Imaging Cholangiopancreatography (See Chapters 16 and 17)
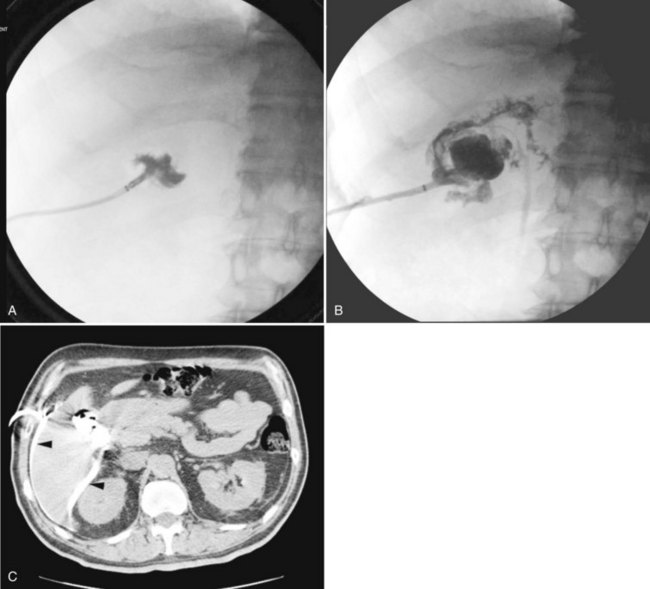
CT and MRCP are better able to show a moderately calcified ectopic gallstone, air in the biliary tree, the presence of additional stones, and a cholecystoduodenal fistula (Swift & Spencer, 1998). CT is useful also for estimating the size of the impacted stone and determining the site of obstruction for planning the operative approach (Fig. 42B.4). Indeed, new multidector CT scanners that use multiplanar or three-dimensional volume-rendering reconstruction will further improve the diagnostic role of CT in detecting fistulae. Already, modern MRI and MRCP scans with improved image resolution and reduced motion artifact have been shown to accuarately detect a small fistulous tract (Chatzoulis et al, 2007). Although such scanning may disclose fusion of the biliary tract to an adjacent viscus, it may not always precisely show a fistula; but MR scanning should be used to show other important pathologic changes, such as distal common duct stones or other obstructive processes, the presence of a subphrenic abscess, pleural effusion, or parasitic disease of the liver (Porta et al, 1981). Scanning also can be used to verify and localize contrast extravasation after interventional procedures, such as PTC or ERCP, or after contrast injection of an existing controlled external fistula (Fig. 42B.5).
Specific Clinical Presentations and Treatment
Gallstone Ileus
The classic plain abdominal film triad of small bowel obstruction, pneumobilia, and ectopic gallstone is considered pathognomonic of gallstone ileus (Rigler et al, 1941); however, the triad is encountered in only 30% to 35% of cases (Balthazar & Schechter, 1978). Pneumobilia is often not appreciated even in retrospect. If biliary-enteric fistula is suspected, and a barium meal is administered, reflux of barium into the biliary tree yields a correct preoperative diagnosis in 60% of patients (Fig. 42B.6). Calculi large enough to obstruct the intestine usually do so in the last 50 cm of ileum, although sometimes also in the jejunum or duodenum and rarely in the sigmoid colon. Such calculi are usually larger than 2.5 cm; if partially calcified, they are readily apparent on a plain radiographs (see Fig. 42B.2B).

Abdominal ultrasound, as mentioned earlier, often establishes the diagnosis of gallstone ileus or provides other information relevant to the diagnosis (Clavien et al, 1990; Davies et al, 1991; Pedersen et al, 1988; Ripolles et al, 2001; Zironi et al, 2007), revealing pneumobilia; the site of the fistula; additional stones still in the gallbladder, or more importantly, in the common duct; and occasionally the location of an ectopic calculus. The diagnositic superiority of CT over abdominal plain films and sonography for gallstone ileus is now well established (Ayantunde & Agarwal, 2007; Lassandro et al, 2005; Loren et al, 1994; Reimann et al, 2004; Swift & Spencer, 1998). In fact, the clinical significance of Rigler’s triad has been revitalized by CT, because all three findings are more consistantly detected (approximately 78%) by this method (Kirchmayr et al, 2005; Ayantunde & Agarwal, 2007; Chou et al, 2007).
The clinical presentation of gallstone ileus has not changed in the past 40 years. In patients with intestinal obstruction, preoperative diagnostic accuracy is approximately 75% (Glenn et al, 1981). Preoperative diagnostic accuracy has contributed to an improved outcome of therapy (Deitz et al, 1986). The increased use of CT in patients with symptoms of intestinal obstruction has led to additional improvement in the diagnostic accuracy of gallstone ileus and has resulted in a decrease in the high mortality rate encountered with this disease (Delabrousse et al, 2000; Lassandro et al, 2004; Reimann et al, 2004; Ayantunde & Agarwal, 2007; Chou et al, 2007).
The terminal ileum is the site of obstruction in 70% of cases (see Figs. 42B.2B and 42B.4B). Unless the obstructed segment is ischemic or has perforated and requires a small bowel resection, the obstructing calculus can be manipulated proximally to a healthy section of bowel, where a safe enterotomy and stone removal may be executed. Jejunal impaction, often by stones larger than 4 cm, occurs approximately 15% of the time, and enterotomy may be made at the site or just proximal to it. Duodenal obstruction, usually in the bulb, is known as Bouveret syndrome (Argyropoulos et al, 1979; Bhama et al, 2002; Cooper & Kucharski, 1978; Koulaouzidis & Moschos 2007; Frattaroli et al, 1997; Maglinte et al, 1987; Thomas et al, 1976), which occurs in 10% of patients and may be handled by duodenostomy or pyloroplasty. It occasionally may be possible to manipulate the stone back into the stomach and remove it via gastrotomy. Rarely, a gastroenterostomy is necessary to protect a duodenotomy or severely traumatized duodenum at the site of impaction.
Bouveret syndrome and other cases of gallstone impaction high in the jejunum have been managed successfully by a combination of endoscopy and electrohydraulic lithotripsy (Fujita et al, 1992; Holl et al, 1989; Moriai et al, 1991; Sackmann et al, 1991). We are aware of one case report of a failed endoscopic extraction that led to spontaneous uneventful passage of the stone (Wagholikar & Ibrarullah, 2004). In rare instances, the sigmoid colon is the site of obstruction of a calculus that has managed to pass through the terminal ileum or enter the colon via a cholecystocolic fistula (Anseline, 1981; Clavien et al, 1990). Almost invariably, some other pathologic process, such as diverticulitis, has produced an area of colonic narrowing. A colostomy is necessary to decompress the proximal bowel. If the impacted stone cannot be manipulated proximally to a transverse colostomy, consideration should be given to exteriorization of the impacted segment with a Hartmann closure of the bowel distal to it (Milsom & MacKeigan, 1985).
Open exploration and enterolithotomy has always been the standard surgical approach for the treatment of classical gallstone ileus. It not only allows removal of the obstructing stone but also permits careful palpation of the entire bowel and gallbladder region, to determine whether other gallstones are in transit more proximally or if any still reside in the diseased gallbladder (see Fig. 42B.2B). These calculi may be poised for passage through the fistula, possibly to induce a recurrent episode of gallstone ileus, a phenomenon estimated to occur in 5% of cases; however, by simple maneuvers, this can be prevented (Clavien et al, 1990; Haq et al, 1981; Levin & Shapiro, 1980). More recently, some authors have described laparoscopic or laparoscopic-assisted treatment for patients with gallstone ileus (Allen et al, 2003; Malvaux et al, 2002; Moberg & Montgomery, 2007; Owera et al, 2008). Because of the limited number of laparoscopically treated patients, it is unclear wherther this approach will reduce the associated high mortality and morbidity rates. Therefore it is our opinion that an open surgical approach should remain the standard of practice and that laparoscopic treatment needs further evaluation.
Considerable debate in the surgical literature surrounds whether cholecystectomy or common duct exploration or both, with dismantling and closure of the cholecystenteric fistula, should accompany enterotomy and relief of the obstruction or await a second operation (Kirchmayr et al, 2005; Muthukumarasamy et al, 2008; Zuegel et al, 1997). Historical data of published reports from the years 1953 through 1993 (Reisner & Cohen, 1994) showed a lower mortality rate of 11.7% in the enterolithotomy-alone group compared with 16.7% for patients who underwent a one-stage operation. Several published reports indicated that operative mortality is lower in these critically ill, elderly patients when only the gallstone obstruction is relieved (Muthukumarasamy et al, 2008; Tan YM et al, 2004; Heuman et al, 1980; Kasahara et al, 1980; VanLandingham & Broders, 1982). This has lead to the general agreement that enterolithotomy alone should be done for fragile patients with significant comorbidities and that the single-stage procedure should be reserved for young, fit, and low-risk patients.
Although some centers have recently published impressively low perioperative mortality rates (0%) for surgical treatment of gallstone ileus, other centers still report rates in the traditional high range (23%; Muthukumarasamy et al, 2008; Tan et al, 2004; Ayantunde & Agarwal, 2007). In a case series from the United Kingdom (Anyantunde & Agarwal, 2007), five deaths occurred in 22 patients; four of the five deaths were patients treated with enterolithomy alone. Seven of 19 patients from YM Tan and colleagues’ (2004) series were clinically unstable and underwent enterolithotomy alone; on long-term follow-up, these patients did not have further complications.
Indeed, careful follow-up of patients treated with enterolithotomy alone indicates that one third to one half will have minimal or no symptoms after relief of the gallstone ileus, and no further treatment will be necessary (Clavien et al, 1990; van Hillo et al, 1987; Tan YM et al, 2004). If a patient has jaundice and intestinal obstruction at the outset, common duct exploration, or at least tube decompression of the common duct, may also be necessary as a lifesaving procedure. For patients who continue to be symptomatic after relief of gallstone ileus, careful preoperative evaluation and bowel preparation can precede a later operation, adding to its safety.
Because common duct stones are found in 40% of patients with biliary-enteric fistula, it is likely that patients who continue to be symptomatic would require endoscopic or open surgical removal of their common duct stones in addition to cholecystectomy and repair of the fistula. As mentioned, operative mortality rate slowly declined to 15% to 25% in large reported series until the early 1970s. Further reductions in operative mortality rates have been possible by limiting treatment to enterotomy and stone removal alone without further surgical therapy in high-risk patients (Ayantunde & Agarwal, 2007; Glenn et al, 1981; Muthukumarasamy et al, 2008; Rodriguez-Sanjuan et al, 1997; Tan YM et al, 2004).
Cholecystoduodenal Fistulae
Most cholecystoduodenal fistulae do not result in gallstone ileus (see Fig. 42B.1A). Rather they are asymptomatic or occur in association with the usual digestive complaints consistent with gastric or biliary tract disease. They may be found during an upper GI barium study or under less welcome circumstances, such as at the time of abdominal surgery for an unrelated problem.
If an asymptomatic or mildly symptomatic cholecystenteric fistula is diagnosed preoperatively, many of the management decisions regarding gallstone ileus discussed previously may apply. Elective surgery may never be necessary in a completely asymptomatic individual, and surgery may present an unfavorable risk-to-benefit ratio in an elderly, minimally symptomatic patient. Along with dismantling of the fistula and common duct exploration, other alternatives to cholecystectomy must be considered, such as a period of expectant management with careful observation, endoscopic papillotomy and stone extraction with the gallbladder left in situ, or interval cholecystectomy if symptoms of pain or cholangitis persist after endoscopic biliary surgery. In a relatively healthy patient younger than 70 years, we believe that open surgical extirpation of the gallbladder, closure of the fistula, and treatment of any common duct pathology promise the best long-term therapeutic result, although some authors advocate laparoscopic treatment of preoperatively diagnosed biliary-enteric fistulae (Chikamori et al, 2001; Crouch & Kuhnke, 2000; Kwon & Inui, 2007; Lee et al, 2004; Rohatgi & Singh, 2006).
If an incidental cholecystoduodenal fistula is discovered at the time of surgery, the major intraoperative decision revolves around the patient’s need for, and ability to tolerate, additional surgical manipulations. If the patient is judged an unsound risk, or if the biliary tract pathology is not believed to be pertinent to the major indication for operation, nothing need be done. Rarely, a cholecystostomy (Fig. 42B.7) and extraction of large calculi can be accomplished with little additional risk. Usually, the gallbladder is shrunken and barely palpable, however, because it is stuck to the duodenum. If the patient can tolerate additional surgery, and sufficient indication exists to proceed at the present operation, rather than at a subsequent one, an attempt should be made to show the biliary-enteric anatomy and state of the common duct by an operative cholangiogram before proceeding with a definitive procedure.
Cholecystocolic Fistulae and Choleric Enteropathy
A cholecystocolonic fistula may develop acutely in patients with long-standing mild or moderately symptomatic biliary tract disease and may be heralded by a sudden change in bowel habits with multiple, loose stools and the development of fever, chills, and other signs of cholangitis from colonic bacterial reflux into the biliary tract. Many elderly patients either weather or ignore these symptoms without seeking medical attention, and some develop signs and symptoms that may incriminate the entire GI tract. Increased stool frequency persists, particularly after ingestion of food, and bouts of fever and malaise subside. Other characteristic symptoms then appear, such as eructation, nausea, weight loss, and increasing diarrhea and steatorrhea. These latter symptoms precede the onset of choleric enteropathy, a dramatic complication of cholecystocolonic fistula. This enteropathy also is seen in other major disturbances of bile acid metabolism, such as with major ileal resection or blind loop syndrome (Brandt, 1984).
Choleric enteropathy comprises of a wide spectrum of anatomic, physiologic, and biochemical changes produced by a significant alteration of the enterohepatic circulation of bile acids. The malabsorption syndrome secondary to cholecystocolonic fistula was clinically documented first by Augur and Gracie (1970) and has since been studied by others (Rau et al, 1980). Ordinarily, 95% of bile acids are passed down the jejunum, aiding in fat and cholesterol absorption, before being largely reabsorbed in the terminal ileum as part of an efficent enterohepatic circulation. Two or three cycles of the bile acid pool per meal occur, with further metabolism of bile acids in the colon and very little lost. With a cholecystocolonic fistula, however, a large part of all of the primary bile acid pool is shunted directly into the colon, resulting in a high luminal concentration of bile acids. In the colon, the primary bile acids undergo deconjugation and dehydroxylation by fecal bacteria, and this increased concentration of bile acids causes a water secretory diarrhea.
Interestingly, only the two natural bile acids with two α-hydroxy groups, chenodeoxycholic acid and deoxycholic acid, induce colonic secretion (Keely et al, 2007). Depending on the amount of bile still passing via the common duct into the small bowel, fat absorption is affected, which over time may result in fatty acid diarrhea. More immediately, however, colonic secretion of water and electrolytes is maximally stimulated by the dihydroxy bile acids. Chenodeoxycholic acid gains access to the colon in large quantities, and massively increased amounts of deoxycholic acid are formed by bacterial dehydroxylation of cholic acid. The primary bile acids and their metabolites are no longer actively absorbed and are lost from the body, eventually causing a chronically lowered bile salt pool beyond the liver’s capacity to synthesize new bile acids to replete it. At this point, even with a partial shunt to the colon, the bile acid concentration still normally passing down the common duct and through the small intestine may be too small to effect micellar solubilization of dietary fat. In contrast to a blind loop syndrome, in which bacterial overgrowth contributes to the choleric enteropathy and can be largely corrected by antibiotics, at least temporarily, cholecystocolonic fistula does not respond adequately to antibiotics. Until the fistula is dismantled, massive shunting of bile acids to the intestine persists and promotes continued watery diarrhea, diminished bile salt pool, and a variable degree of fat malabsorption.
Cholangitis seems to be a more prominent feature of cholecystocolonic fistula, when the fistula is narrow and prone to intermittent obstruction of bile flow (Edell et al, 1981; Safaie-Shirazi et al, 1973), whereas diarrhea with a lesser incidence of fever and chills is more common with a wide-open fistula (Lygidakis, 1981); we are also aware of one case report of a patient with a cholecystocolonic fistula who was seen with massive lower GI hemorrhage (Kunasani et al, 2003). In any instance, a fistula to the colon is more likely than other biliary-enteric fistulae to have associated cholangitis; if it does, the serum levels of bilirubin, alanine aminotransferase, and γ-glutamyltransferase may be slightly elevated and may direct attention to the biliary and upper digestive tract.
Because of the unusual initial complaints, full investigations for malabsorption that include upper GI studies, GI sonography, and jejunal biopsy may be undertaken but usually do not clarify the diagnosis. A pathognomonic triad consisting of pneumobilia, chronic diarrhea, and vitamin K malabsorption was recently suggested by Savvidou and colleagues (2009) to aid in the diagnosis of cholecystocolonic fistula. Diversion of bile acids into the colon results in malabsorption of fat and fat-soluble vitamins. In particular, vitamin K deficiency can be clinically significant and is easily detected by a prolonged prothrombin time (PT), and it can be corrected by parenteral supplementation (Savvidou et al, 2009). Although the condition of bile acid malabsorption can be easily diagnosed by the selenium-75-homocholic acid taurine (SeHCAT) test, this study is time consuming and is not widely available (Pattni & Walters, 2009). Plain abdominal radiographs have been reported to reveal air in the biliary tree in only 50% of cases, however, the diagnosis becomes evident only if a barium enema examination is done, preferably with air contrast, because barium (Fig. 42B.8) and air fill the gallbladder and extrahepatic bile ducts. In a recent report, a barium enema showing contrast filling of the biliary tract was used to diagnose a patient with a rare choledochocolonic fistula causing severe diarrhea (Anees et al, 2008). Failure of even a barium enema to show a cholecystocolonic fistula has been reported, but this is quite rare. In such cases, the cholecystocolic fistula is diagnosed by ERCP (Arvanitidis et al, 2004; Schoeters et al, 2002).
There is little controversy about the appropriate treatment for cholecystocolic fistulae. Except in the most extenuating circumstances, the fistulae should be dismantled because of the ever-present risk of sepsis. If the diagnosis can be made preoperatively, suitable mechanical and antibiotic bowel preparation reduces the chance of infectious complications of surgery and aids primary closure of the large bowel. Cholecystectomy and, if indicated, common duct exploration should be done at the same time. Centers with significant expertise in laparoscopic surgery have reported successful treatment of preoperatively diagnosed cholecystocolonic fistulae by this method (Chatzoulis et al, 2007; Gentileschi et al, 1995; Hida et al, 1999; Lee et al, 2004; Wang et al, 2006). Regardless of the choice of surgical treatment, preoperative ERCP with sphincterotomy and stone extraction may obviate the need to explore the CBD and, in rare cases, might result in spontaneous closure of the fistula, obviating surgery altogether (Marshall et al, 1990).
Cholecystocholedochal Fistula, Including Mirizzi Syndrome
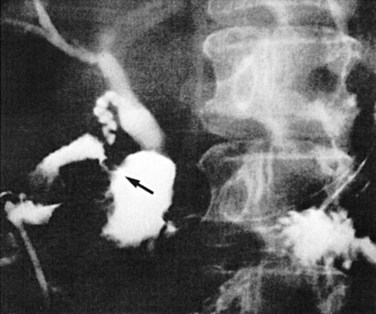
The pathogenesis of cholecystobiliary fistula is similar to the mechanism of fistula formation between the gallbladder and other adjacent segments of the alimentary tract: the offending calculus remains impacted in the ampulla of the gallbladder or cystic duct, and the resultant inflammation causes adherence and then perforation into the adjacent structure (see Fig. 42B.1D) In 1948, Mirizzi described the clinical picture in detail and called it functional hepatic syndrome. It is now commonly referred to as Mirizzi syndrome (see Chapters 29 and 43). The mechanism of jaundice was postulated by Mirizzi to be due to spasm of the hepatic sphincter secondary to inflammation in the region of the cystic duct junction with the common hepatic duct (Mirizzi, 1948); however, extensive histologic studies have failed to disclose a “sphincter” in the common hepatic duct. The large size of the stone and the acute cholecystitis with marked pressure necrosis and inflammatory reaction at the site of stone intrusion into the common hepatic duct combine to produce jaundice with variable components of extrinsic compression and intrinsic calculous blockage of bile flow.
The early phase of this cholecystobiliary fistula presumably exists when a large gallstone is impacted in the ampulla of the gallbladder or in the intramural segment of the cystic duct, which often courses parallel to the common duct. The jaundice that occurs as a consequence of this pathologic anatomy is clinically indistinguishable from choledocholithiasis. McSherry and colleagues (1982) suggested that this classic picture (Fig. 42B.9) of Mirizzi’s “functional hepatic syndrome” be subclassified as type 1. With progression of the disease, extrusion of the stone into the common hepatic duct may occur, and a fistula may form between the gallbladder and the hepatic duct. This is classified as type 2 (see Fig. 42B.1D), which is characteristically diagnosed intraoperatively by observing a gush of bile on removal of the impacted stone, indicating a biliobiliary fistula. Csendes and colleagues (1989) further subclassified type 2 patients into three categories based on the percentage of the wall of the common duct that was eroded by the offending calculus. In this subclassification, type II is a fistula involving less than one third of the circumference of the bile duct, type III involves two thirds, and type IV is a fistula with complete bile duct destruction. This classification scheme was recently updated to include a type V, which describes cholecystoenteric fistula, with or without gallstone ileus, coexisting with any of the other types (Csendes et al, 2007).
The large and solitary nature of the ampullary and cystic duct stones may be a hint to the preoperative diagnosis. The classic findings on ultrasonography include dilation of the biliary system that includes the common hepatic duct above the gallbladder neck, a stone impacted in the gallbladder, and an abrupt change in the caliber of the common duct below the stone (Hayek et al, 1988). Because most of these patients present with jaundice or some abnormalities on LFTs, a preoperative ERCP or PTC frequently is performed. These imaging studies permit a precise delineation of the condition, markedly altering surgical strategy. Cornud and others (1981) showed the appearance of biliobiliary fistulae at PTC, whereas Heil and Belohlavek (1978) relied on ERCP. In the six patients documented by McSherry and colleagues (1982), PTC and ERCP were equally effective in elucidating the cause of common duct obstruction. Although MRCP has been shown to diagnose Mirizzi syndrome preoperatively, it is limited, because it rarely shows the fistula and does not afford therapeutic stenting (Rappeport, 2002).
Biliobiliary fistulae have been referred to as a “trap” in the surgery of cholelithiasis (Corlette & Bismuth, 1975
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
 Portal hypertension in children
Portal hypertension in children
 Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
 Bile duct exploration and biliary-enteric anastomosis
Bile duct exploration and biliary-enteric anastomosis
 Recurrent pyogenic cholangitis
Recurrent pyogenic cholangitis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


