Fig. 20.1
Patient and team positioning
20.2.2 Beginning of RPLS
The umbilicus is incised (Fig. 20.2), and the fascia opened until to reach the peritoneum, which is opened as well. A purse-string suture using PDS 1 is placed in full-thickness method in the umbilical fascia and peritoneum at 2, 4, 6, 8, 10, 12 o’clock positions (Fig. 20.3). An 11-mm reusable metallic trocar is introduced into the peritoneal cavity inside the purse-string suture, and the pneumoperitoneum is created (Fig. 20.4). A 10-mm, 30° rigid and standard length scope (Karl Storz-Endoskope) is advanced through the 11-mm trocar, and curved reusable instruments according to DAPRI (Karl Storz-Endoskope) are inserted into the abdomen through the umbilical scar without trocars. The bicurved grasping forceps III (Fig. 20.5) is inserted through a separate fascia window, created by a sharp obturator of 5-mm trocar, at some of 5 mm outside the purse-string suture at 10 o’clock position in the respect of the patient head (Fig. 20.6). The other instruments like the monocurved coagulating hook (Fig. 20.7a), the monocurved scissors (Fig. 20.7b), the monocurved bipolar grasping forceps and scissors (Fig. 20.7c, d), the bicurved needle holder II (Fig. 20.7e), the monocurved suction and irrigation cannula, the straight 5-mm clip applier, and the straight 5-mm grasping forceps are introduced on the other side of the bicurved grasping forceps III at 3 o’clock position, parallel to the 11-mm trocar and inside the purse-string suture (Fig. 20.8). The suture is adjusted to maintain a tight seal around the 5-mm tools and the 11-mm trocar, and open only for the change of the instruments and evacuation of the smoke created with the dissection. The operative table is positioned in a reversed Trendelenburg position.

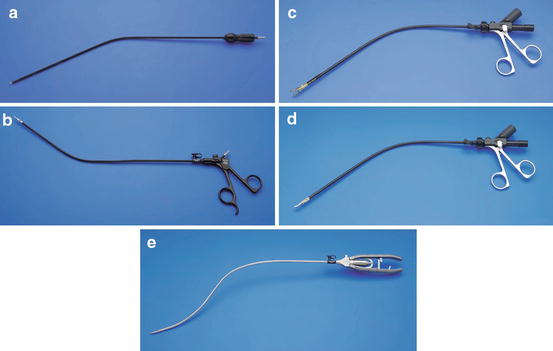
Fig. 20.2
Transumbilical access: incision of the original umbilical scar
Fig. 20.3
Transumbilical access: placement of the purse-string suture (PDS 1) in the umbilical fascia and peritoneum at 2, 4, 6, 8, 10, 12 o’clock positions
Fig. 20.4
Transumbilical access: insertion of the 11-mm reusable metallic trocar
Fig. 20.5
Bicurved reusable grasping forceps III according to DAPRI (Karl Storz-Endoskope)
Fig. 20.6
Transumbilical access: insertion of the grasping forceps III through a separate fascia window at some of 5 mm outside the purse-string suture at 10 o’clock position
Fig. 20.7
Other curved reusable instruments according to DAPRI (Karl Storz-Endoskope): monocurved coagulating hook (a), monocurved scissors (b), monocurved bipolar grasping forceps (c), monocurved bipolar scissors (d), bicurved needle holder II (e)
Fig. 20.8
Transumbilical access: insertion of the other curved instruments at 3 o’clock position, parallel to the 11-mm trocar and inside the purse-string suture
The distal curve of the bicurved grasping forceps III is used to retract the left liver lobe and to contemporary expose the opening of the hepatogastric ligament on the lesser curvature (Fig. 20.9a, b). Thanks to the peculiar shape of the instruments, the scope never appeared in conflict with the instruments’ tips, and the conflict between the surgeon’s hands and the scope is avoided.
Fig. 20.9
Use of the distal curve of the bicurved grasping forceps III to retract the left liver lobe and to contemporary expose the opening of the hepatogastric ligament (a), without any conflict between the surgeons’ hands (b)
If an insufficient exposure of the hiatal region is evidenced, the DAPRI 1.8-mm trocarless grasping forceps (Fig. 20.10) is inserted percutaneously under the xyphoid access, through a skin puncture created by a Veress needle (Fig. 20.11). This grasper is placed under the left liver lobe and against the diaphragm.
Fig. 20.10
1.8-mm trocarless grasping forceps according to DAPRI (Karl Storz-Endoskope)
Fig. 20.11
Placement of the DAPRI 1.8-mm trocarless grasping forceps percutaneously under the xyphoid access
The hepatogastric ligament is opened close to the liver segment 1, and the right phrenogastric ligament is incised as well (Fig. 20.12), dividing its anterior and posterior sheets. The right crus is freed from bottom to top (Fig. 20.13). The left phrenogastric ligament is incised (Fig. 20.14), and the left crus is exposed. The lower esophagus is freed, encircled and suspended by a piece of cotton tape using the bicurved grasping forceps III (Fig. 20.15a, b). Thanks to this maneuver, both crura under the esophagus are better exposed and more easily freed (Fig. 20.16).
Fig. 20.12
Incision of the right phrenogastric ligament using the coagulating hook
Fig. 20.13
Skeletonization of the right crus using the coagulating hook from bottom to top
Fig. 20.14
Incision of the left phrenogastric ligament using the coagulating hook
Fig. 20.15
Suspension of the lower esophagus by a piece of cotton tape (a) using the bicurved grasping forceps III and the straight 5-mm grasping forceps (b)
Fig. 20.16
Easier mobilization of both crura thanks to the cotton tape’s tension
The operative table is maintained in a reversed Trendelenburg position with right-sided tilt, permitting an increased exposure of the splenic region. The gastrosplenic ligament is incised starting from the previous dissection of the left phrenogastric ligament, until to control the first short gastric vessel (Fig. 20.17). Then, the operative table is replaced without any tilt and maintaining the Trendelenburg position, in order to move the upper part of the gastric fundus behind the lower esophagus. The other short gastric vessels are just dissected “à la demand” giving a more slack to the wrap (Fig. 20.18a, b), using the monocurved coagulating hook or the monocurved bipolar grasping forceps and scissors.