have been destroyed by the tubular alterations. An escape of Tamm-Horsfall (uromodulin) protein from damaged collecting tubules into the interstitium has been demonstrated in about 50% of patients with NPHP-MCKD as a periodic acid-Schiff (PAS)-positive material and by specific immunofluorescence staining with an anti-THP antibody.8 Immunofluorescence does not otherwise contribute to the diagnosis of NPHP-MCKD.
TABLE 15.1 Shared and Distinguishing Features Among Diseases of the NPHP-MCKD Complex | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
For the recessive forms the term nephronophthisis (NPHP) is used, whereas the designation medullary cystic kidney disease (MCKD) denotes the dominant variants of the complex (Table 15.1B[i]).10,11
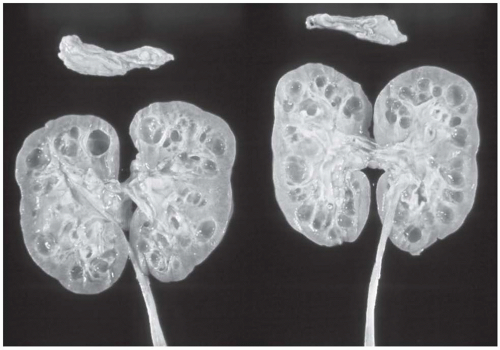 FIGURE 15.1 Juvenile nephronophthisis (autopsy case, 13-year-old girl). Note the numerous cysts of varying size in the medulla and at the corticomedullary junction. (Reproduced with permission from Hildebrandt F, Waldherr R, Kutt R, et al. The nephronophthisis complex: clinical and genetic aspects. Clin Invest 1992;70:802.) |
of hyperuricemia and gout in MCKD123 and MCKD2.22 MCKD2 patients with UMOD mutations also may exhibit defects in urine concentrating ability.24 Recently, an extensive study on genotype-phenotype correlations in mutation of NPHP genes has been published.25 NPHP1 can occur in combination with ocular motor apraxia Cogan type,26,27 with retinitis pigmentosa in Senior-Løken syndrome (SLSN),20 with liver fibrosis28 with cone-shaped epiphyses in Mainzer-Saldino syndrome,29 and with coloboma of the optic nerve and cerebellar vermis aplasia in Joubert syndrome type B (JBTSB) (Tables 15.1B[iii] and 15.2).30 Infantile NPHP (type 2) can be associated with situs inversus31 and one case report describes a patient with a nonsense inversin mutation with retinitis pigmentosa.32 NPHP4 patients may have retinitis pigmentosa (SLSN) and Cogan syndrome.33 NPHP5 patients display early onset retinitis pigmentosa (SLSN) in all known cases.20 NPHP6 and NPHP8 patients have SLSN, Joubert syndrome, or Meckel-Gruber syndrome (MKS).25,34,35 NPHP9 is associated with SLSN.36 NPHP10 patients display SLSN and Bardet-Biedl syndrome (BBS)-like phenotypes,37 whereas patients with NPHP11 show JBTS, MKS, and liver fibrosis.38,39 NPHP12 patients exhibit Jeune asphyxiating thoracic dystrophy.40
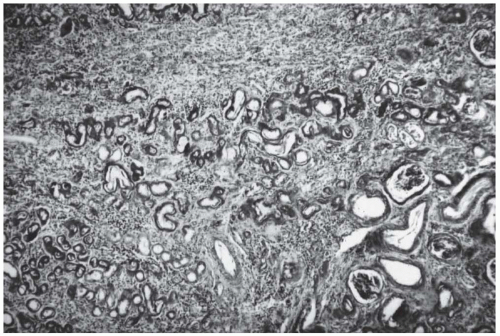 FIGURE 15.2 Renal histology in juvenile nephronophthisis (NPHP1). Note the characteristic triad, which consists of (1) tubular basement membrane disintegration with thickening as well as attenuation of the tubular basement membrane, (2) interstitial round cell infiltration with marked fibrosis, and later on (3) tubular atrophy and cyst development. (Courtesy of Prof. R. Waldherr, Heidelberg, Germany.) |
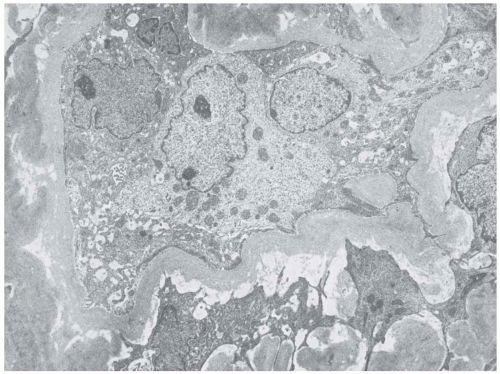 FIGURE 15.3 Thickening, wrinkling, and double layering of tubular basement membranes with intermembranous fibroblasts and dedifferentiation of tubular epithelial cells. An electron micrograph. (Reproduced with permission from Hildebrandt F, Waldherr R, Kutt R, et al. The nephronophthisis complex: clinical and genetic aspects. Clin Invest 1992;70:802.) |
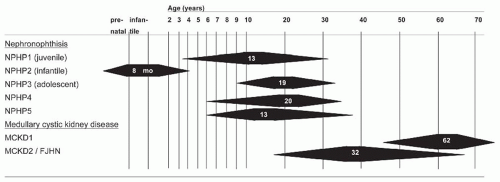 FIGURE 15.4 The time course of renal failure in NPHP-MCKD. Range for age of onset of end-stage renal disease is shown as solid triangles. Numbers indicates median age in years. NPHP, nephronophthisis; MCKD, medullary cystic kidney disease; FJHN, familial juvenile hyperuricemic nephropathy. |
Inversin localizes to primary cilia, mitotic spindles, and centrosomes74 and is intimately associated with the microtubule cytoskeleton.75 INVS/NPHP2 mutations remain a rare cause of NPHP, accounting for <1% of cases.
TABLE 15.2 Disease Variants, Gene Loci, and Extrarenal Involvement in the NPHP-MCKD Complex of Diseases | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


