Fig. 19.1
Cosmetic result of a representative Technique II case
19.2 Technique I: Extragastric Approach
19.2.1 Setup
The patient is placed in a supine position with legs spread apart. The surgeon stands between the patient’s legs, and the assistant surgeon stands on the right side of the patient to hold the laparoscope. The scrub nurse stands on the left side (Fig. 19.2).

Fig. 19.2
The main surgeon stands between the patient’s legs. The multichannel port called x-Gate® (Sumitomo Bakelite) is placed under the navel via a 2.5-cm incision
19.2.2 Establishment of the Main Access Route
A 2.5-cm longitudinal incision is made at the navel. The ligament beneath the navel is incised. The fascia is opened with a 2.5-cm longitudinal incision so that the peritoneum is incised for entry into the abdominal cavity. The inner ring of a multichannel port, x-Gate® (Sumitomo Bakelite, Tokyo, Japan) (Fig. 19.3) [6], is inserted into the abdominal cavity. The inner ring of the port is brought close to the outer ring by pulling up the four belts attached to the inner ring. This manipulation also enlarges the opening in the abdominal wall as the belts force the parietal incision to expand from the inside. The converter is then attached to the outer ring of the main unit by rotating it clockwise. A long 5-mm cannula and a short 5-mm cannula are inserted through the channels on the cephalic side of the converter. To complete establishment of the access port, the gas supply tube is connected to one cannula, and the smoke evacuation tube is connected to the other. We use a 5-mm long-shafted laparoscope with a forward viewing angle of 30° and to which a high definition charge-coupled device camera is attached (Karl Storz-Endoskope, Tuttlingen, Germany).

Fig. 19.3
The main body of x-Gate® (Sumitomo Bakelite) consists of a hard outer ring and a flexible inner ring. The converter has four flexible channels, one of which one allows 12-mm instruments
19.2.3 Insertion of 2-mm Forceps
BJ Needle® (Niti On Co., Chiba, Japan) (Fig. 19.4) is a very thin-caliber grasping forceps with a shaft diameter of 2 mm. The access port specially manufactured for BJ Needle® (BJ Port® (Niti On Co.)) is inserted into the abdominal cavity. The puncture site depends on the tumor location and the surgeon’s preference. Generally, the left upper quadrant is chosen. BJ Needle® (Niti On Co.) is rigid enough to manipulate the stomach and surrounding tissue with adequate traction and expose the target.

Fig. 19.4
A 2-mm grasper (BJ needle® (Niti On Co.)), which adds remarkable assistance in reduced port surgery, helps preserve the cosmetic appearance of the port-site wound
19.2.4 Resection
We limit use of a stapling device to tumors that protrude well outside the stomach. This is because resection of a tumor with a stapling device can remove too much of the healthy gastric wall, which results in severe stomach deformity. Moreover, when the tumor is located at the lesser curvature, resection with a stapling device can damage the vagal nerve and thus cause gastric dysmotility [7, 8].
When the tumor is identified, traction is exerted on the gastric wall with the BJ needle® (Niti On Co.), and another forceps is inserted through one of the x-Gate® channels (Sumitomo Bakelite) (Fig. 19.5a). For this, we usually use a 5-mm bendable grasper (Diamond Flex®, Snowden Spencer, USA). With the two graspers, appropriate tension is applied to the target point on the gastric wall, which is incised with SonoSurg® (Olympus, Tokyo, Japan), a reusable ultrasonically activated device. When the margin of the tumor is not clearly identifiable on the serosal aspect, intraoperative peroral gastroscopy is performed to identify the safety margin from inside. Full-thickness resection of the stomach wall containing the tumor is performed. The procedure involves only minimal resection of healthy tissue around the tumor (Fig. 19.5b). The specimen is enclosed in a retrieval bag (Fig. 19.5c).
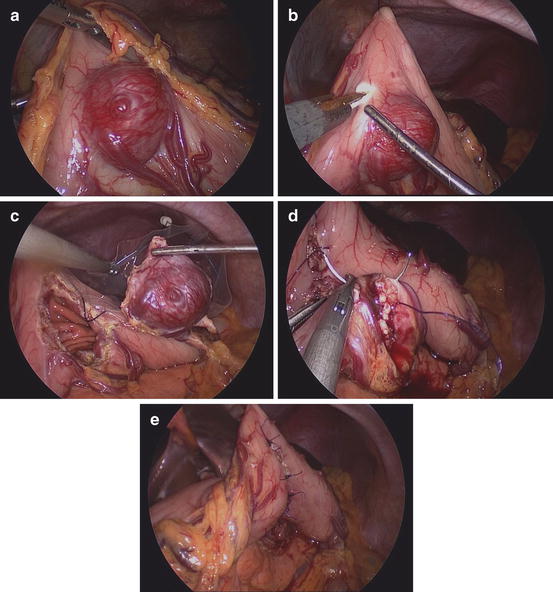
Fig. 19.5
(a) To expose the submucosal tumor, effective traction is applied to the stomach with a bendable grasper and a needle grasper. (b) The tumor, with an adequate safety margin, is removed by full-thickness gastric resection with an ultrasonically activated device. (c) The resected specimen is captured in an extraction bag. (d) The defect is closed by suturing. The full-thickness is approximated by a continuous running suture with absorbable 3-0 monofilament material. (e) The seromuscular layer is closed with interrupted sutures
19.2.5 Closure of the Defect
The full-thickness defect on the gastric wall is closed by manual suturing. We use a “parrot jaw” needle grasper (Karl Storz-Endoskope), which is inserted through the x-Gate® (Sumitomo Bakelite) and driven by the left hand, and a BJ needle® (Niti On Co.) as an assistant forceps held in the right hand. Absorbable monofilament 3-0 suture with a 26-mm half-circle needle is used. The x-Gate® channels (Sumitomo Bakelite) are flexible enough to facilitate swift insertion and withdrawal of the 26-mm needle.
The suture line is completed transversely, crossing the longitudinal axis of the stomach at a right angle. The idea is to avoid stenosis. The full thickness of the gastric wall is first closed by continuous running suture (Fig. 19.5d), and the seromuscular layer is then approximated by interrupted suture (Fig. 19.5e). After closure, peroral gastroscopy is performed to confirm hemostasis, smooth passage, and peristalsis.
The retrieval bag containing the specimen is brought out through the navel. We usually do not leave any drainage tube. The wounds are closed in a cosmetic manner.
19.2.6 Tips and Tricks
19.2.6.1 Turning the Stomach Over
When the tumor is located in the posterior wall of the stomach, the stomach must be turned over. To achieve this, the greater omentum is divided caudal to the gastroepiploic vessels, and the greater curvature is stitched at an appropriate point with a 3-0 thread and a straight needle. The needle is pushed through the abdominal wall into the abdomen. It penetrates the stomach wall, finally returning to the abdominal wall. Both ends of the thread are pulled up or loosened extracorporeally to control the degree of traction (Fig. 19.6). There are several alternative devices, such as EndoGrab® (Virtual Ports Ltd., Caesaera, Israel), [9]), an internal retractor that can be used to turn the stomach.










