Fig. 7.1
Vector of forceps movement in laparoscopic cholecystectomy. In RPLS, the forceps are in coaxial becomes with the scope. (CLS conventional laparoscopic surgery, RPLS reduced port laparoscopic surgery)
When the left and right forceps are inserted through the same port, the angle between the forceps is reduced to less than 10° at the surgical site [4] and the principle of triangulation, established in CLS, is violated. As a result, when traction must be applied to tissue, the forceps are usually manipulated in a cephalad to caudal or anterior to posterior direction. Use of these instruments in SPLS can also result in interference between the handles and unwanted contact within the abdominal cavity, termed “clashing” and “sword fighting.” Interference is also commonly seen between scope and ultrasonically activated device (USAD), vessel sealing system (VSD), and/or irrigation and suction device (Fig. 7.2).
Fig. 7.2
Clashing: clashing occurs because the forceps and scope are located within a limited space
7.3 Techniques for Avoiding Clashing and Sword Fighting
RPLS requires considerable adjustment to avoid interference when a multi-channel access device is inserted through the limited area of the navel. Here are some important points to remember.
7.3.1 Scopes
CLS commonly uses a rigid scope angled at 30° or 45°. The standard scope is approximately 30 cm in length and has an eyepiece attached to a camera head and light guide cable. The light guide cable is ordinarily positioned perpendicular to the scope. In RPLS, the light guide cable and camera head can interfere with the operating forceps, making it difficult to maintain a clear visual field.
Use of a longer scope is one option for reducing interference between the scope and forceps. Recently, scopes for bariatric surgery have come onto the market, including a 45-cm scope from Stryker Corporation (Kalamazoo, MI, USA) and a 50-cm scope from Karl Storz-Endoscope (Tuttlingen, Germany) (Fig. 7.3). With these scopes, the camera head and light guide cable can be moved away from the hand that operates the forceps, reducing interference.
Fig. 7.3
A 50-cm long, 5-mm rigid scope and 90° light adapter (Karl Storz-Endoscope)
In particular, the light guide cable can interfere with forceps manipulation. This is because the cable is positioned perpendicular to the scope. Such interference can be avoided by using a light adapter angled at 90° (Fig. 7.4).
Fig. 7.4
The flexible scope can be used to establish a suitable distance between the forceps and the handheld scope
The use of a flexible scope requires less space between the hand operating the scope and the hand operating the forceps. The Olympus LTF-S19-5 (Olympus Medical Systems Co., Tokyo, Japan) is a flexible hi-vision scope 5.4-mm in diameter (Fig. 7.5) that maintains a clear visual field while reducing clashing.

Fig. 7.5
LTF-S19-5 deflectable videoscope (Olympus). The tip of the scope can be moved 200° in four directions and the CCD/ light-guide cables are arranged in one line
7.3.2 Trocars
Two or more trocars can be inserted directly through a single incision in the abdominal wall (multiple trocar approach). This permits the effective use of conventional tools in SPLS. However, only limited space is available for trocar positioning. The use of three to four conventional trocars can result in clashing of their housings, which interferes with accurate forceps manipulation. Such clashing can be avoided if we vary the trocar length (Fig. 7.6a). By using three trocars of different lengths (5-, 10-, and 15-cm), clashing can be reduced or eliminated.
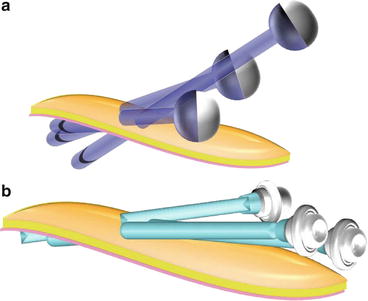
Fig. 7.6
Trocar housing clashes are prevented by (a) use of different sleeve lengths (ex. 5-, 10- and 15-cm) and (b) use of small housings (low-profile trocars)
Another approach is to use trocars with smaller housings. These “low-profile” trocars also effectively reduce clashing (Fig. 7.6b). A number of brands are currently on the market (Fig. 7.7).
Fig. 7.7
Low-profile trocars. (a) Versaport Bladeless Optical Trocar (Covidien). (b) Linaport (LINA Medical). (c) E•Z Trocar Smart Insertion II (Hakko). (d) Slender port (TOP)
7.3.3 Access Ports
The multi-trocar approach can make it difficult to consistently insert the trocars in the appropriate positions, and it is subject to differences among surgeons. In addition, the location of the inner tip is difficult to confirm upon insertion of a second and third trocar. The use of a multi-channel port, in comparison to the multi-trocar approach, facilitates easier insertion of instruments developed for SPLS. Ordinarily, the port is inserted through a 2- to 4-cm skin incision.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


